

Alimentary System
Tongue - Inflammation
Narrative
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
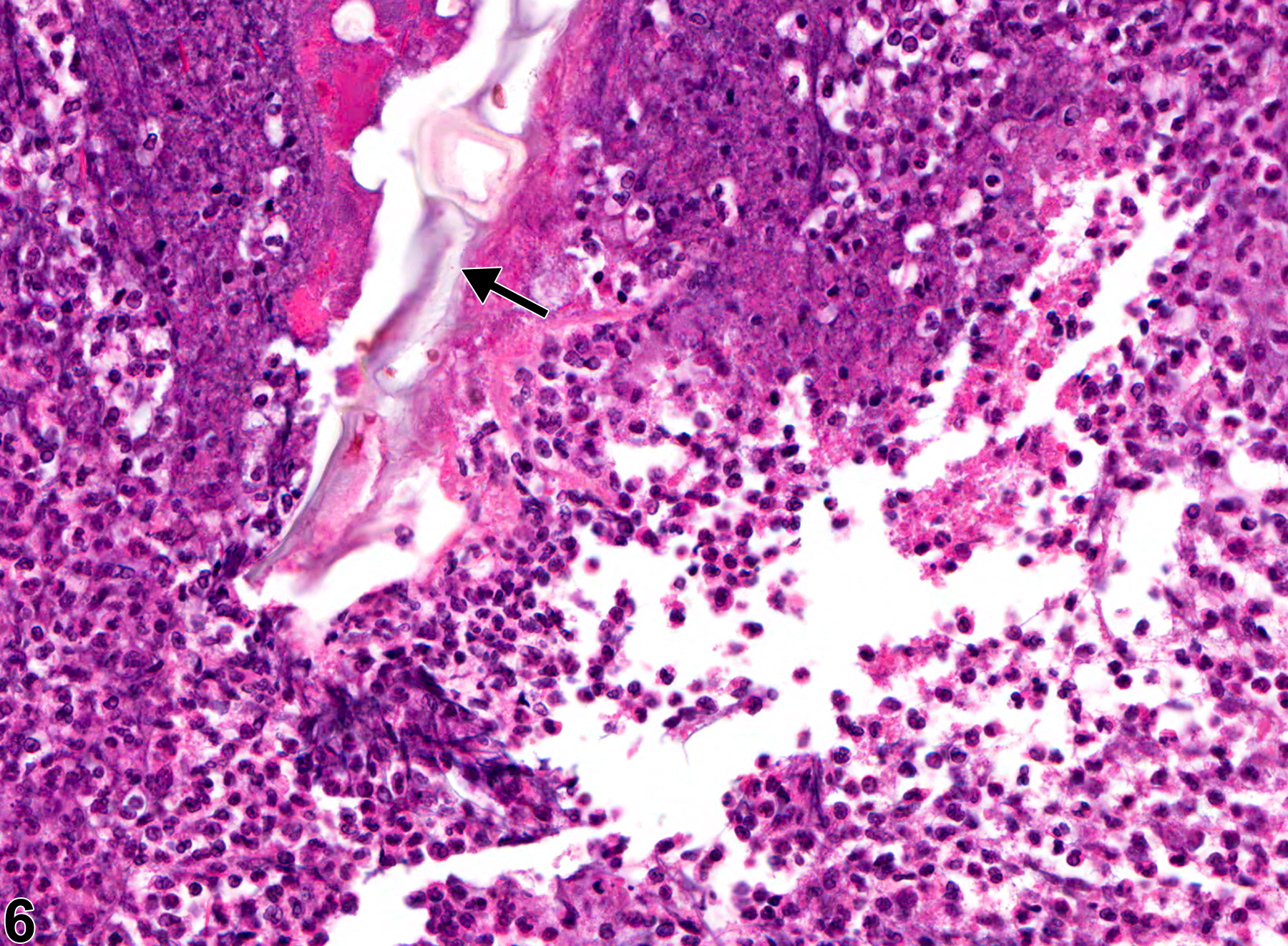
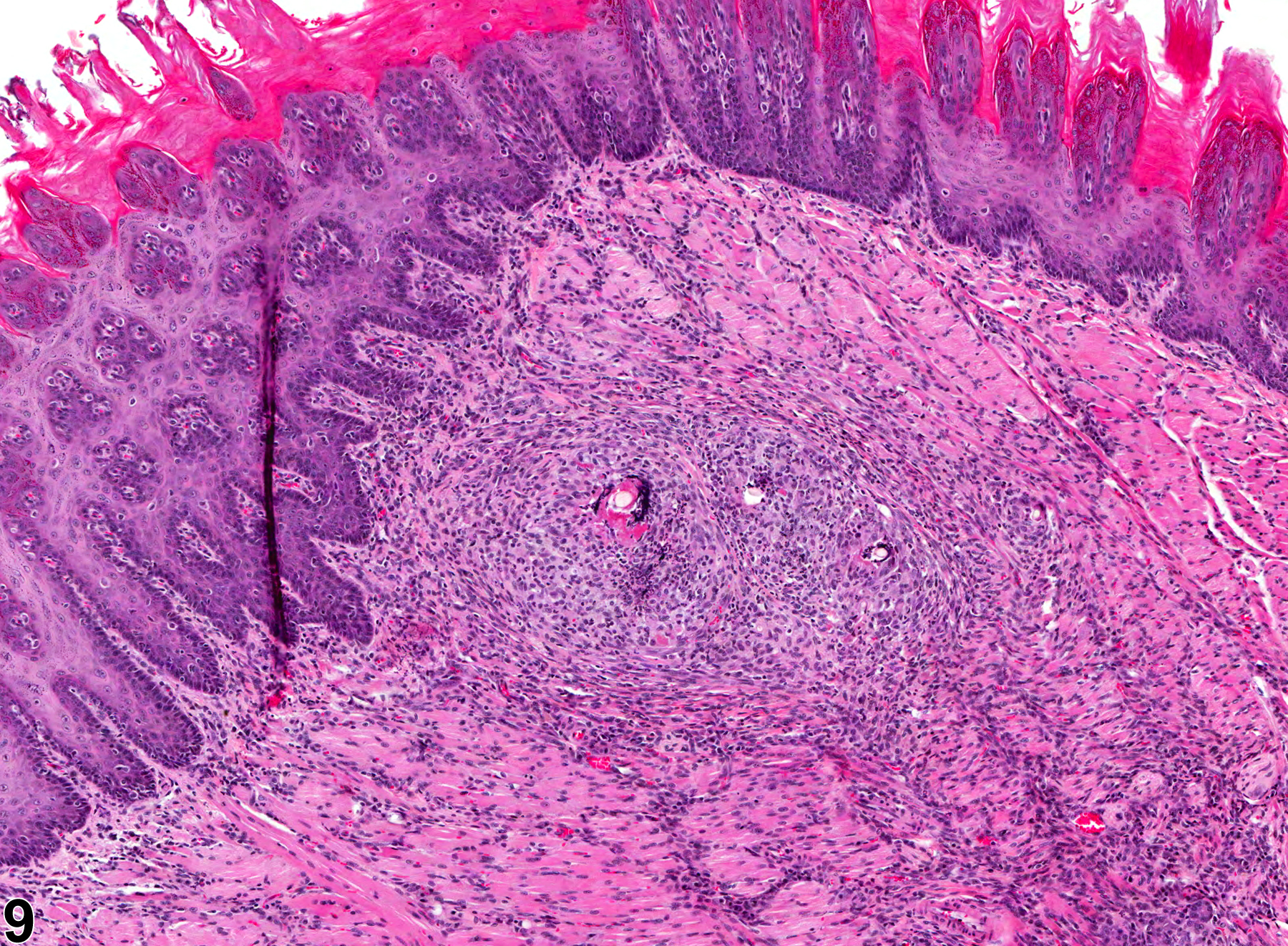
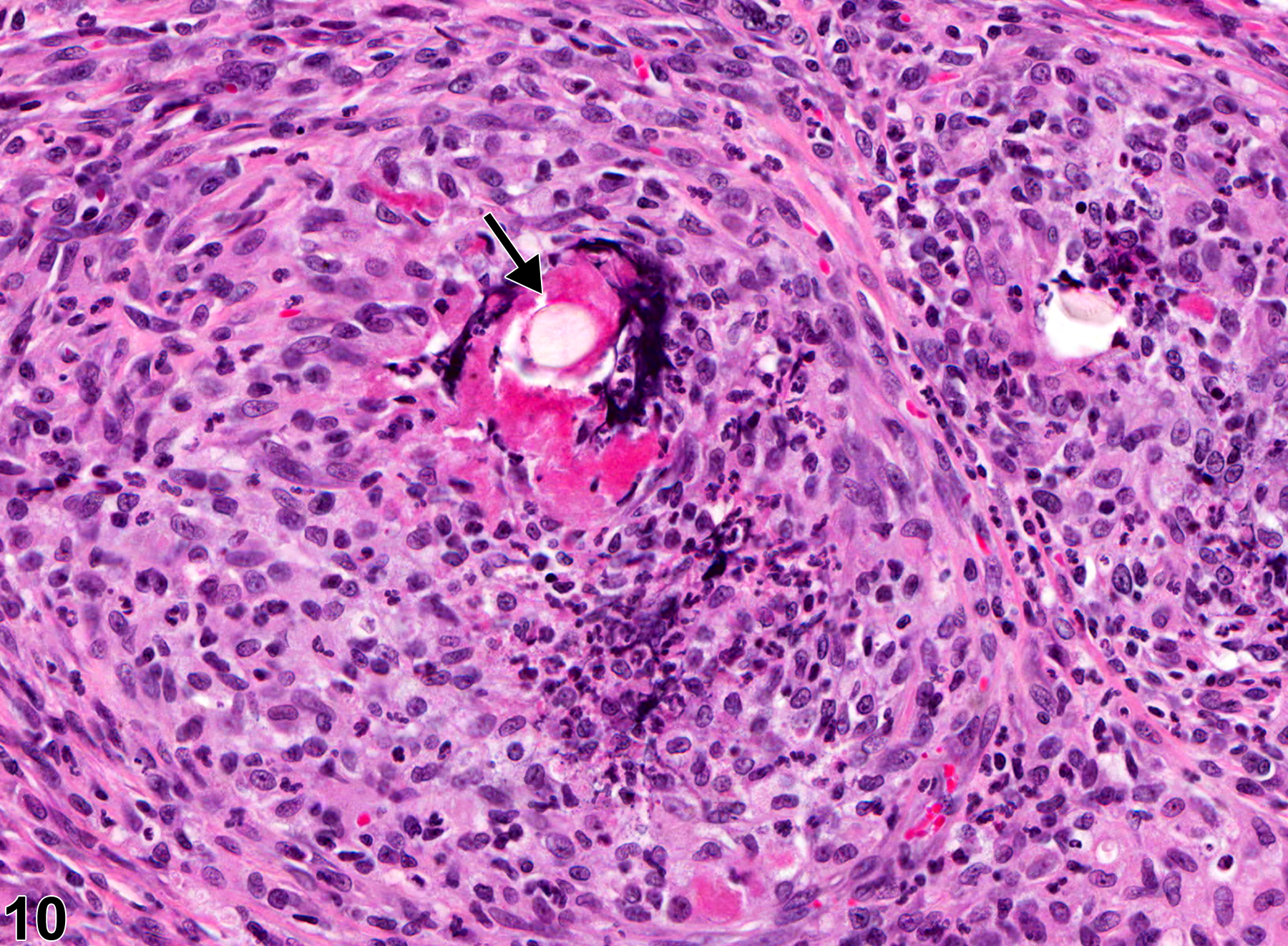
Inflammation can be a treatment-related lesion but can also occur as a spontaneous background lesion. Suppurative inflammation is often due to foreign bodies (Figure 6) or bacterial infections. If the inciting agent persists (e.g., the foreign body is not removed), the inflammatory response may become granulomatous (Figure 9 and Figure 10). The NTP uses the term "suppurative inflammation" for lesions that are considered abscesses. Generally, abscesses are incidental findings; however, a treatment-related increased incidence could occur with agents toxic to the squamous epithelium of the tongue.
Ackermann MR. 2007. Chronic inflammation and wound healing. In: Pathologic Basis of Veterinary Disease, 4th ed (McGavin MD, Zachary JF, eds). Mosby, St Louis, MO, 101-152.
Bertram TA, Markovits JE, Juliana MM. 1996. Non-proliferative lesions of the alimentary canal in rats GI-1. In: Guides for Toxicologic Pathology. STP/ARP/AFIP, Washington, DC, 1-16.
Full Text: https://www.toxpath.org/docs/SSNDC/GINonproliferativeRat.pdfBrown HR, Hardisty JF. 1990. Oral cavity, esophagus and stomach. In: Pathology of the Fischer Rat (Boorman GA, Montgomery CA, MacKenzie WF, eds). Academic Press, San Diego, CA, 9-30.
Abstract: https://www.ncbi.nlm.nih.gov/nlmcatalog/9002563Greaves P. 2007. Digestive system. In: Histopathology of Preclinical Toxicity Studies, 3rd ed. Academic Press, London, 334-456.
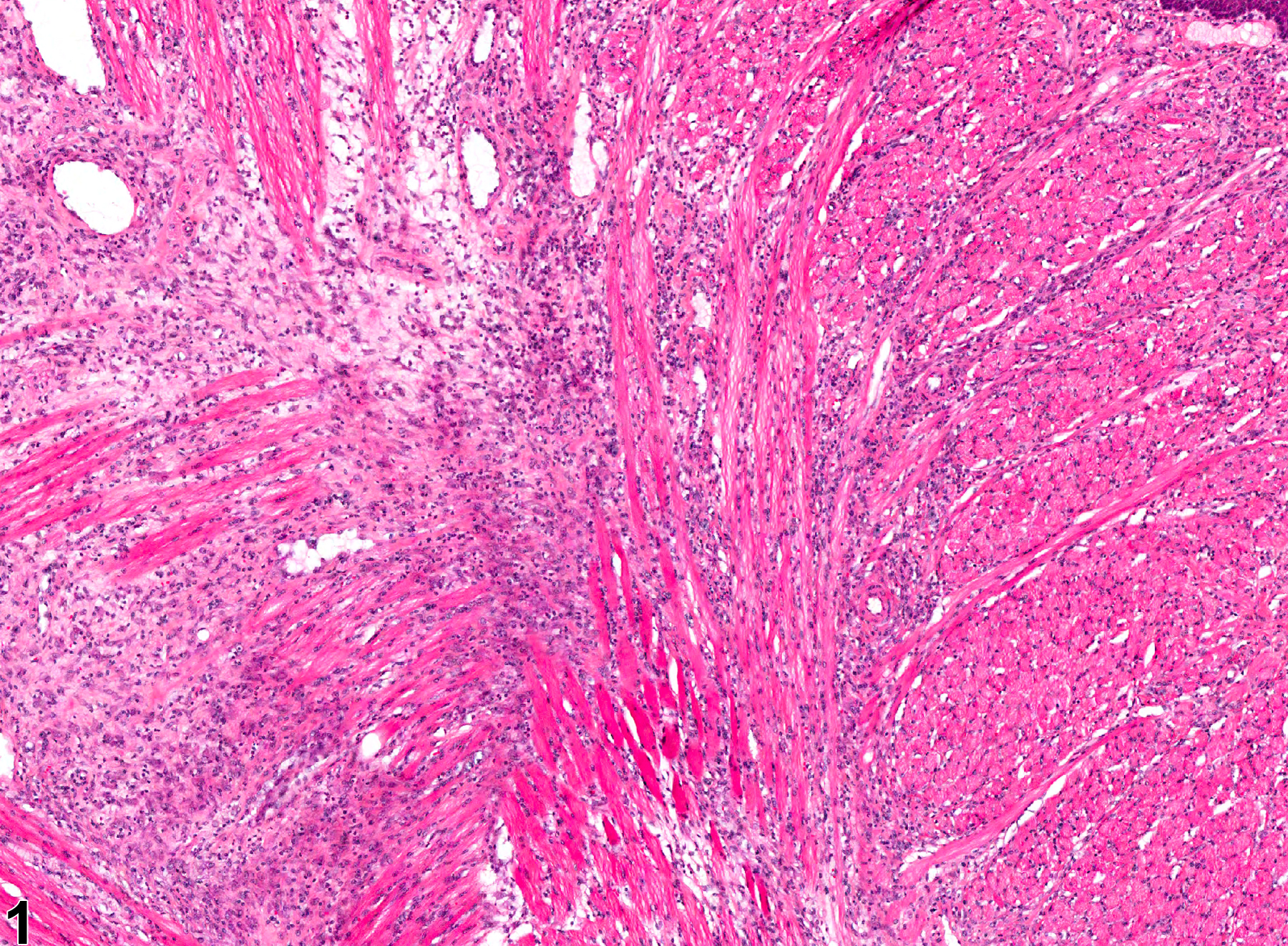
Tongue - Inflammation, Chronic active in a male F344/N rat from a chronic study. The muscle bundles are separated by inflammatory cells and fluid.
All Images

Tongue - Inflammation, Chronic active in a male F344/N rat from a chronic study. The muscle bundles are separated by inflammatory cells and fluid.

Tongue - Inflammation, Chronic active in a male F344/N rat from a chronic study (higher magnification of Figure 1). Inflammatory cells comprise lymphocytes, macrophages, and neutrophils.

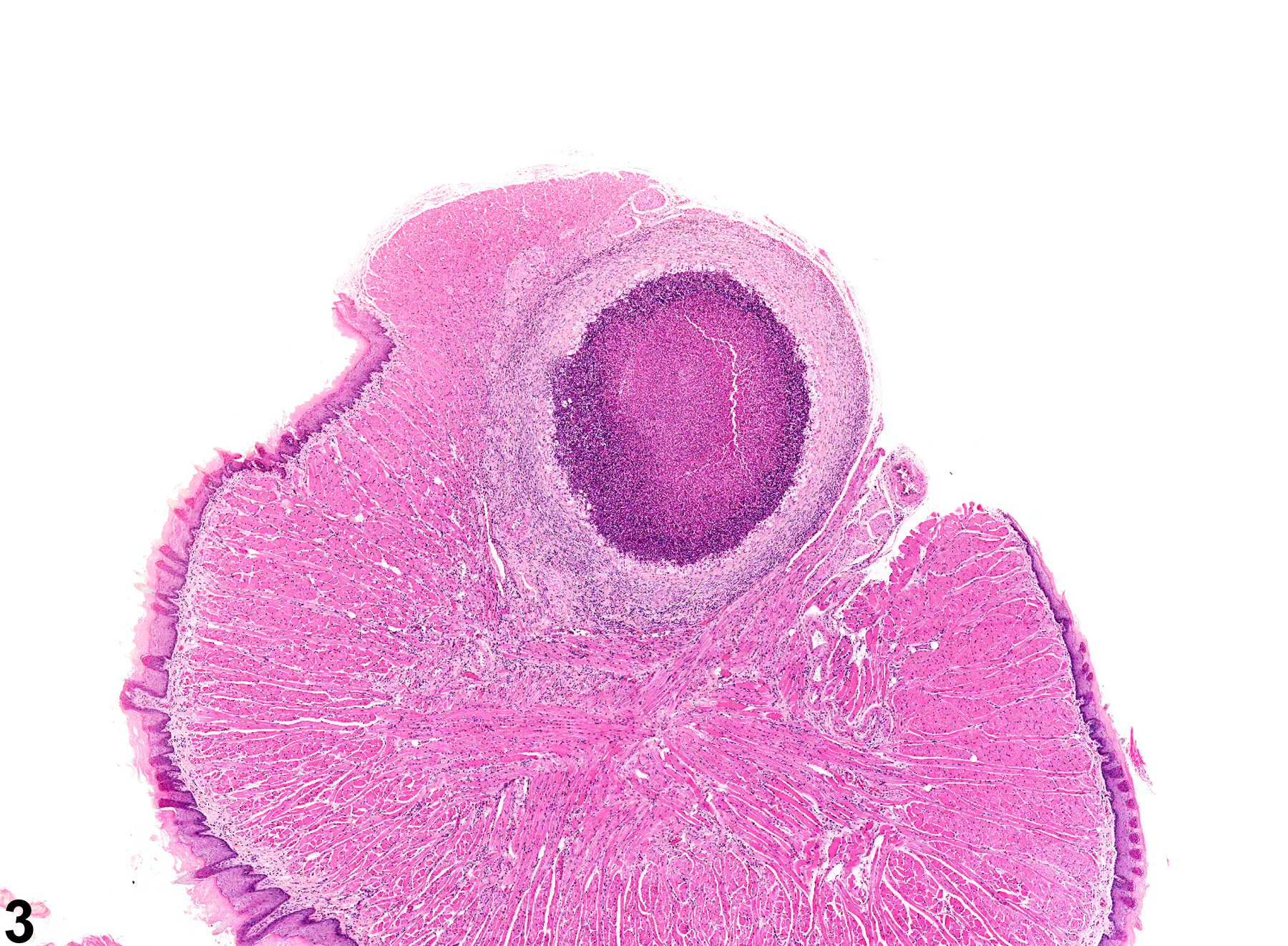
Tongue - Inflammation, Suppurative in a female F344/N rat from a chronic study. There is a large abscess in the tongue.

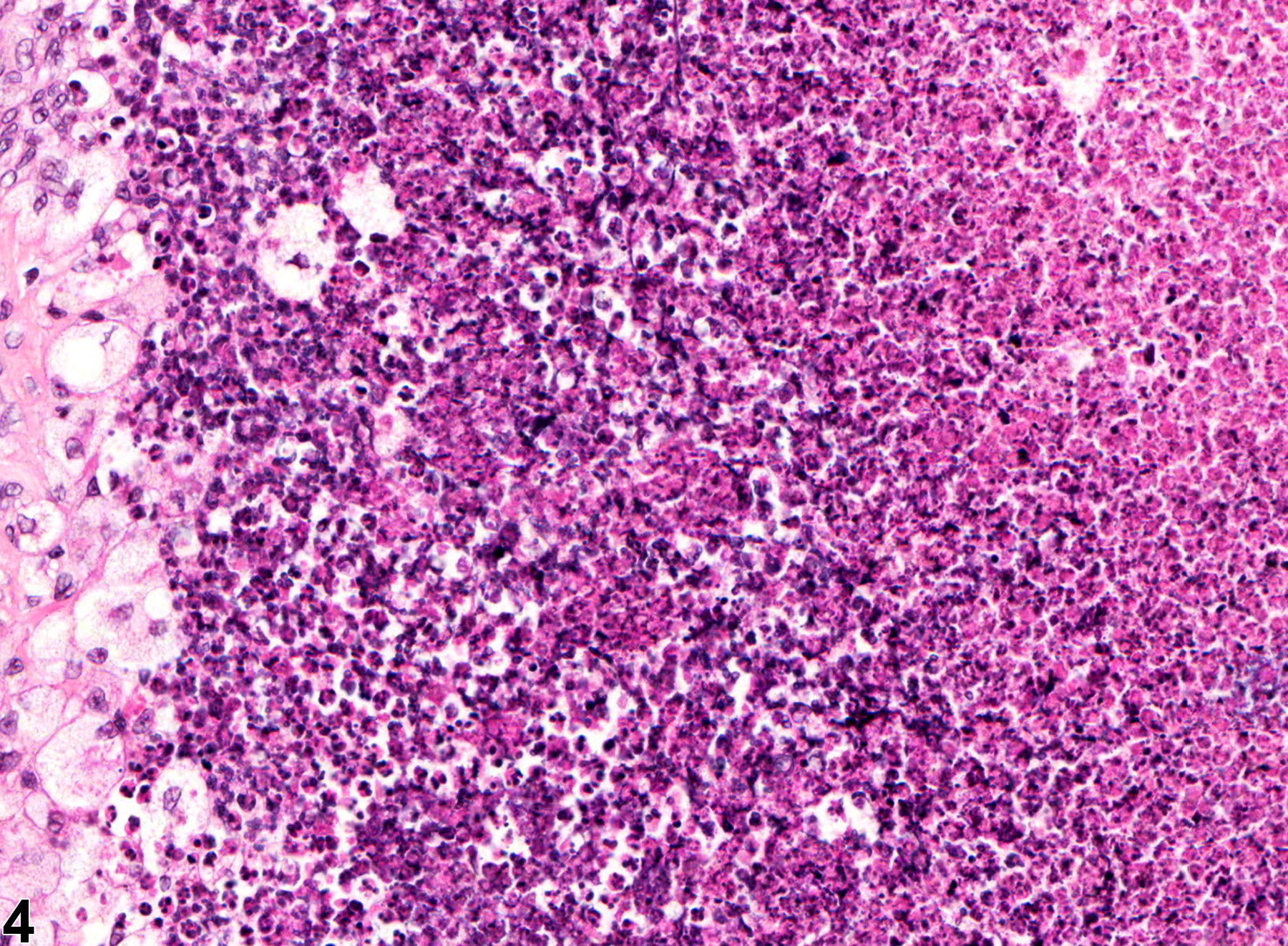
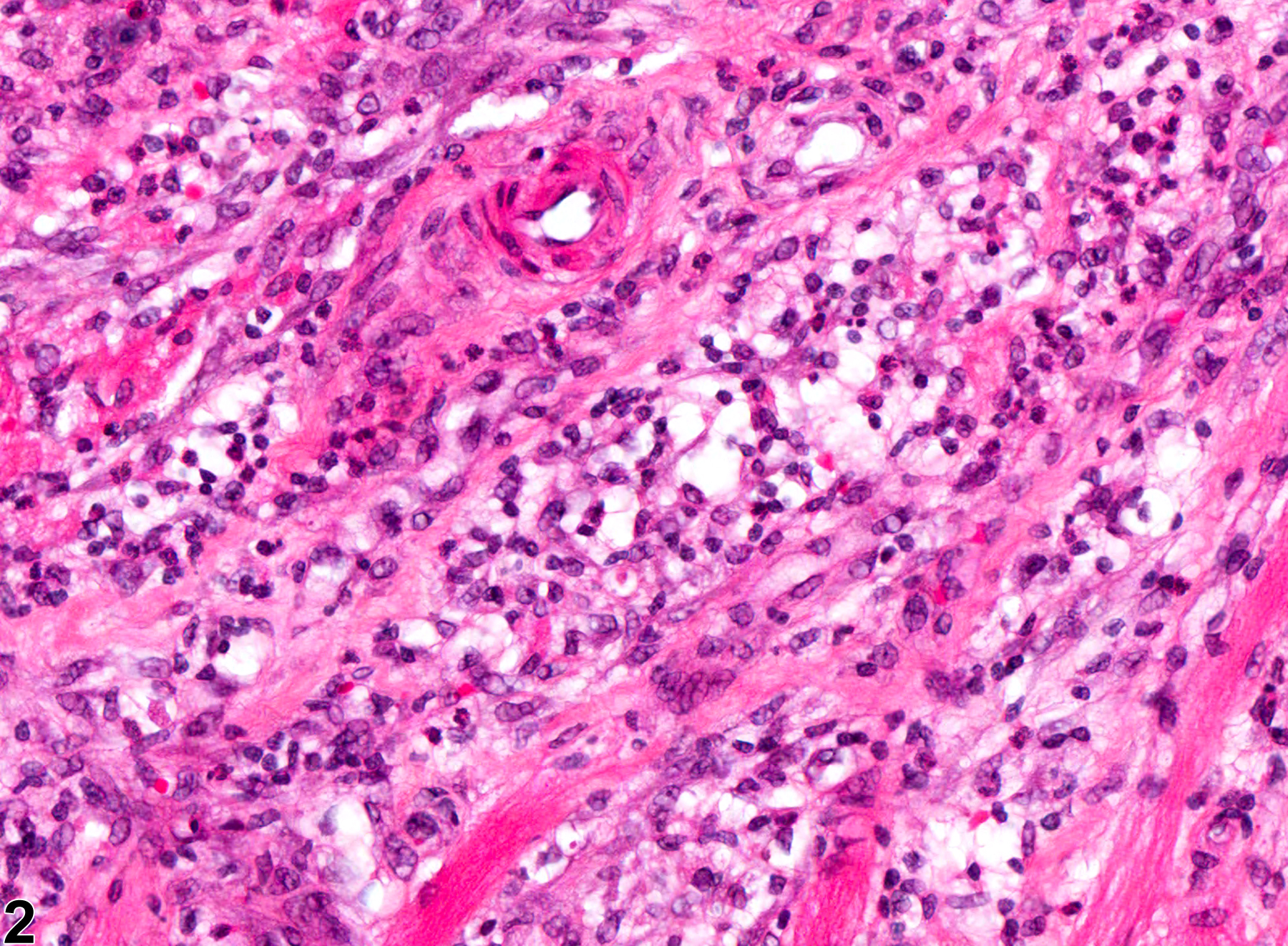
Tongue - Inflammation, Suppurative in a female F344/N rat from a chronic study (higher magnification of Figure 3). The center of the abscess is composed of degenerate neutrophils and cellular debris and is surrounded by large, activated macrophages, lymphocytes, and fibrous connective tissue.

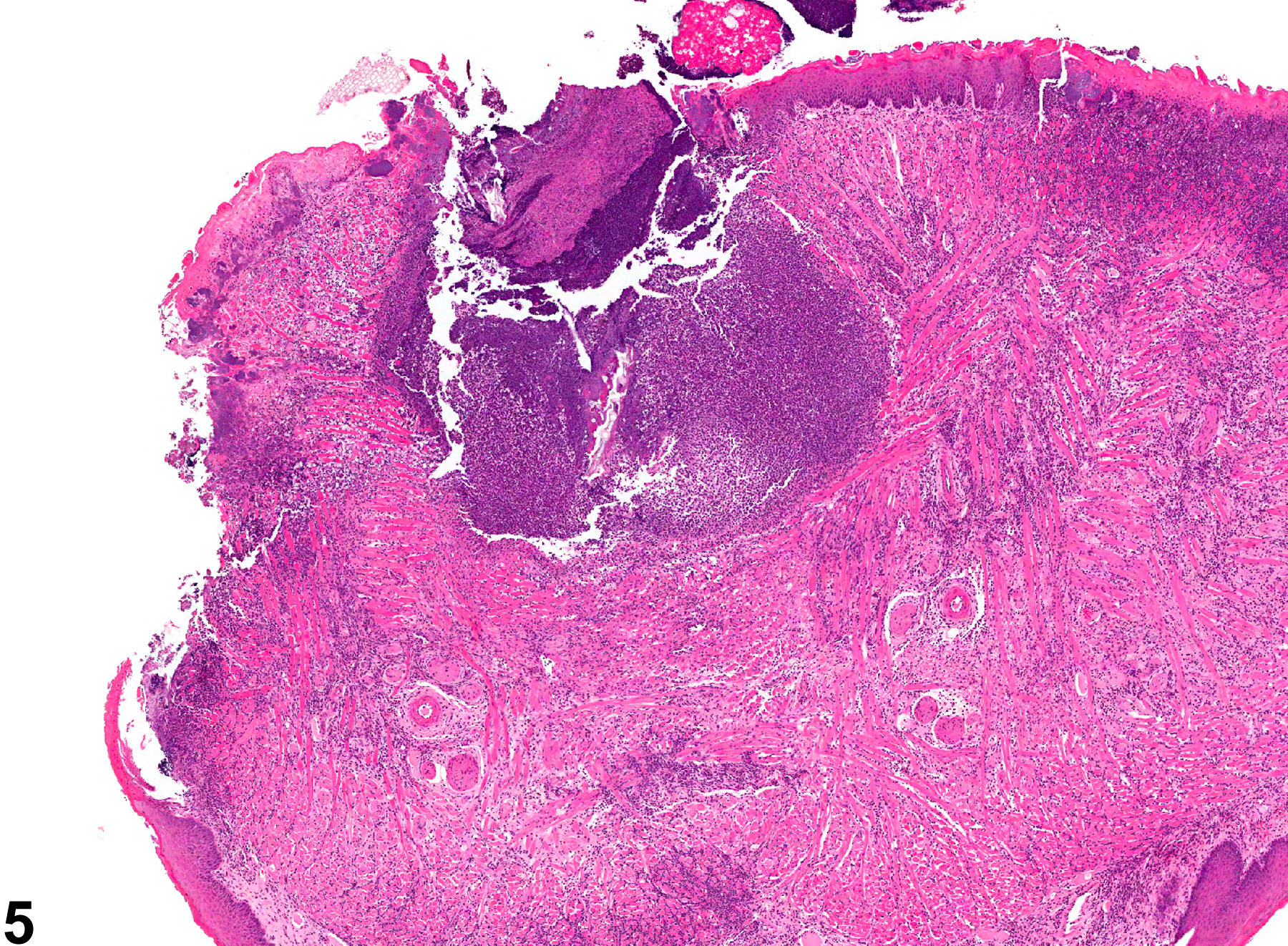
Tongue - Inflammation, Suppurative in a male Swiss CD-1 mouse from a chronic study. There is a large, abscess in the tongue.

Tongue - Inflammation, Suppurative in a male Swiss CD-1 mouse from a chronic study (higher magnification of Figure 5). The center of the abscess is composed of degenerate neutrophils and cellular debris and contains a fragment of foreign material (arrow).

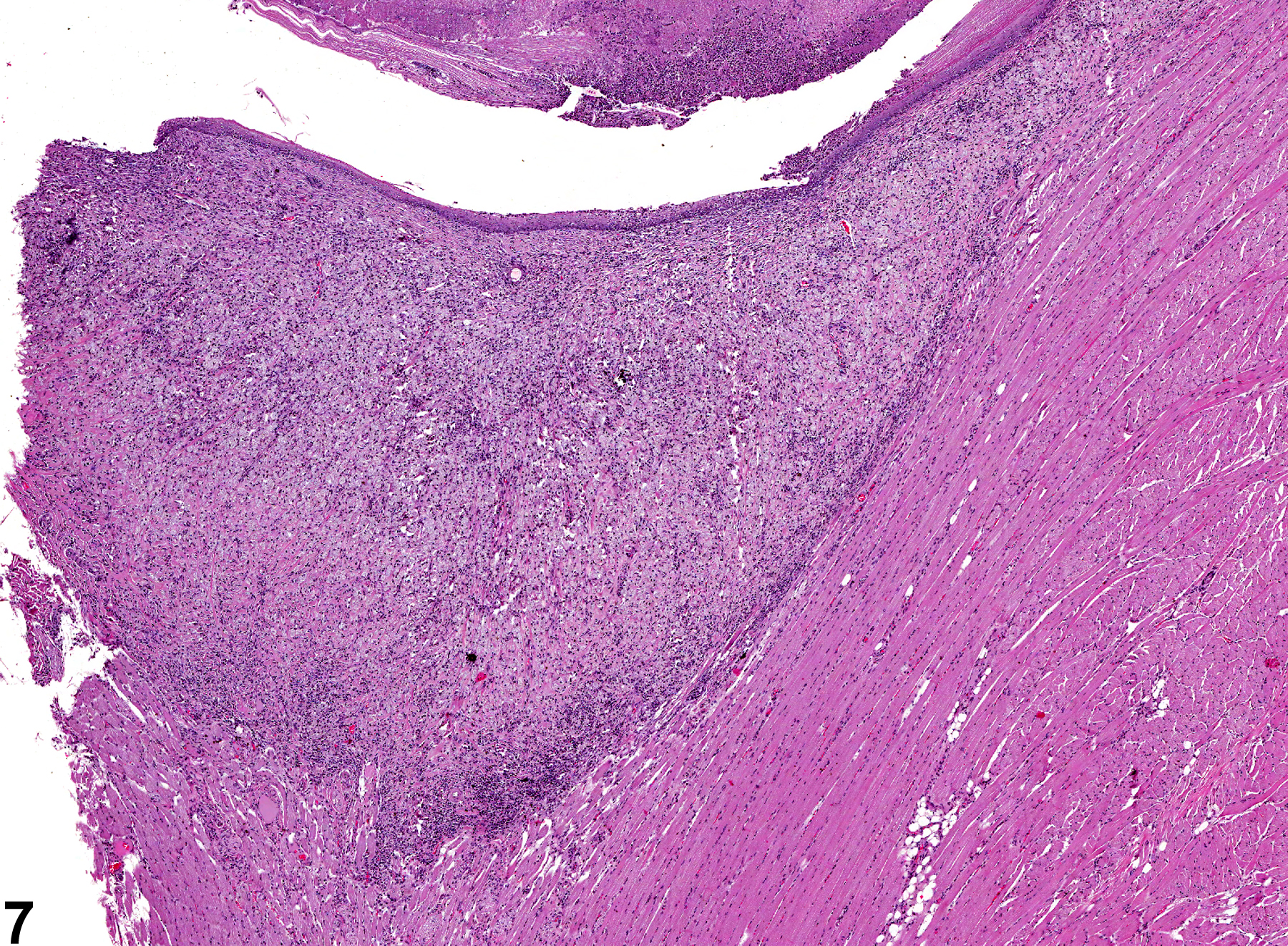
Tongue - Inflammation, Granulomatous in a female F344/N rat from a chronic study. There is a large, subepithelial area of inflammation.

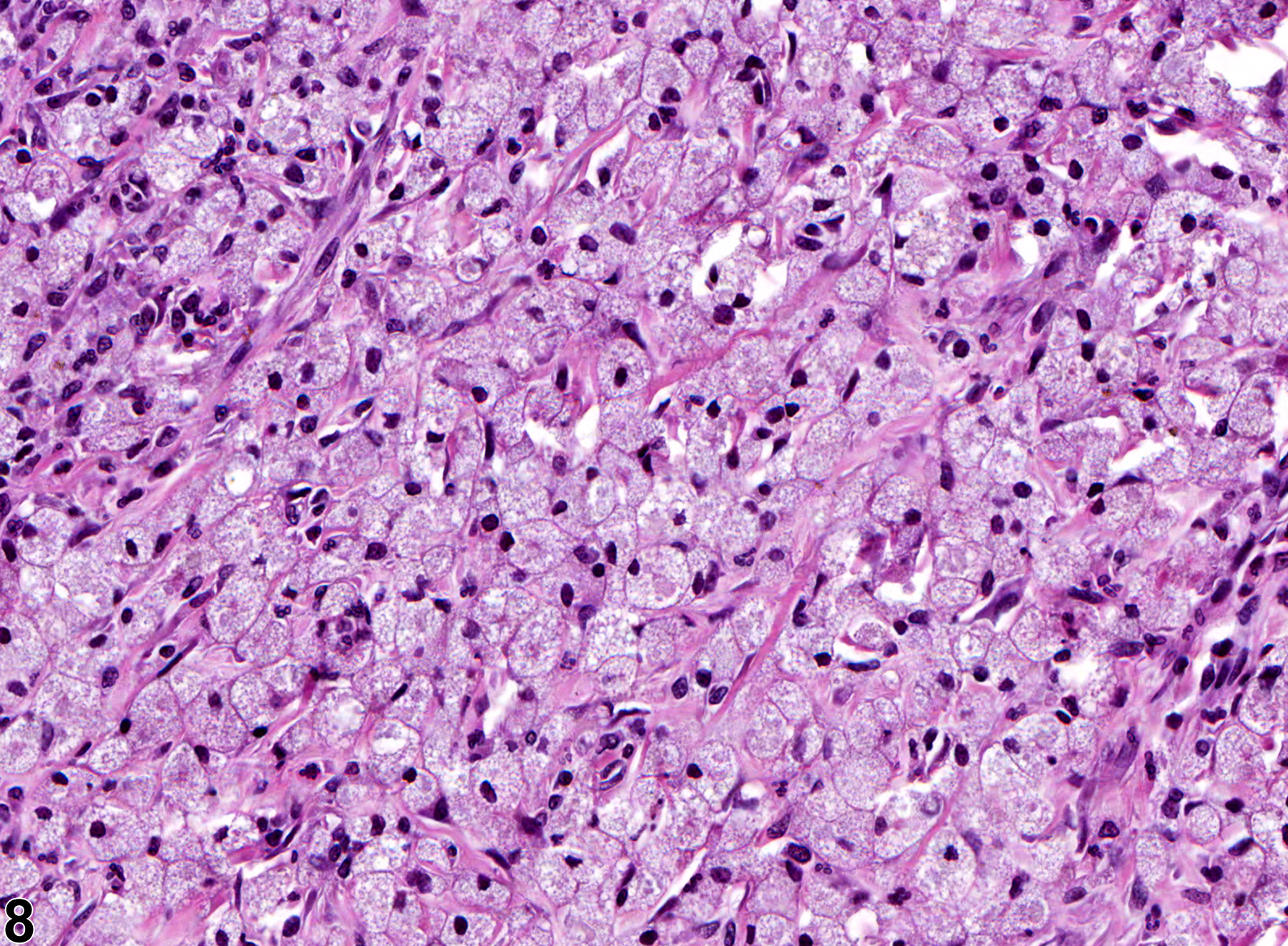
Tongue - Inflammation, Granulomatous in a female F344/N rat from a chronic study (higher magnification of Figure 7). The majority of the inflammatory cells are large, epithelioid macrophages, with fewer lymphocytes and neutrophils.

Tongue - Inflammation, Granulomatous in a male Swiss CD-1 mouse from a chronic study. There is a subepithelial focus of inflammation in the tongue.

Tongue - Inflammation, Granulomatous in a male Swiss CD-1 mouse from a chronic study (higher magnification of Figure 9). The center of the inflammatory focus is composed of epithelioid macrophages with fewer neutrophils and lymphocytes and contains a hair shaft (arrow).