

Endocrine System
Adrenal Gland, Cortex - Hypertrophy
Narrative
{kind=link}
{kind=link}
{kind=link}
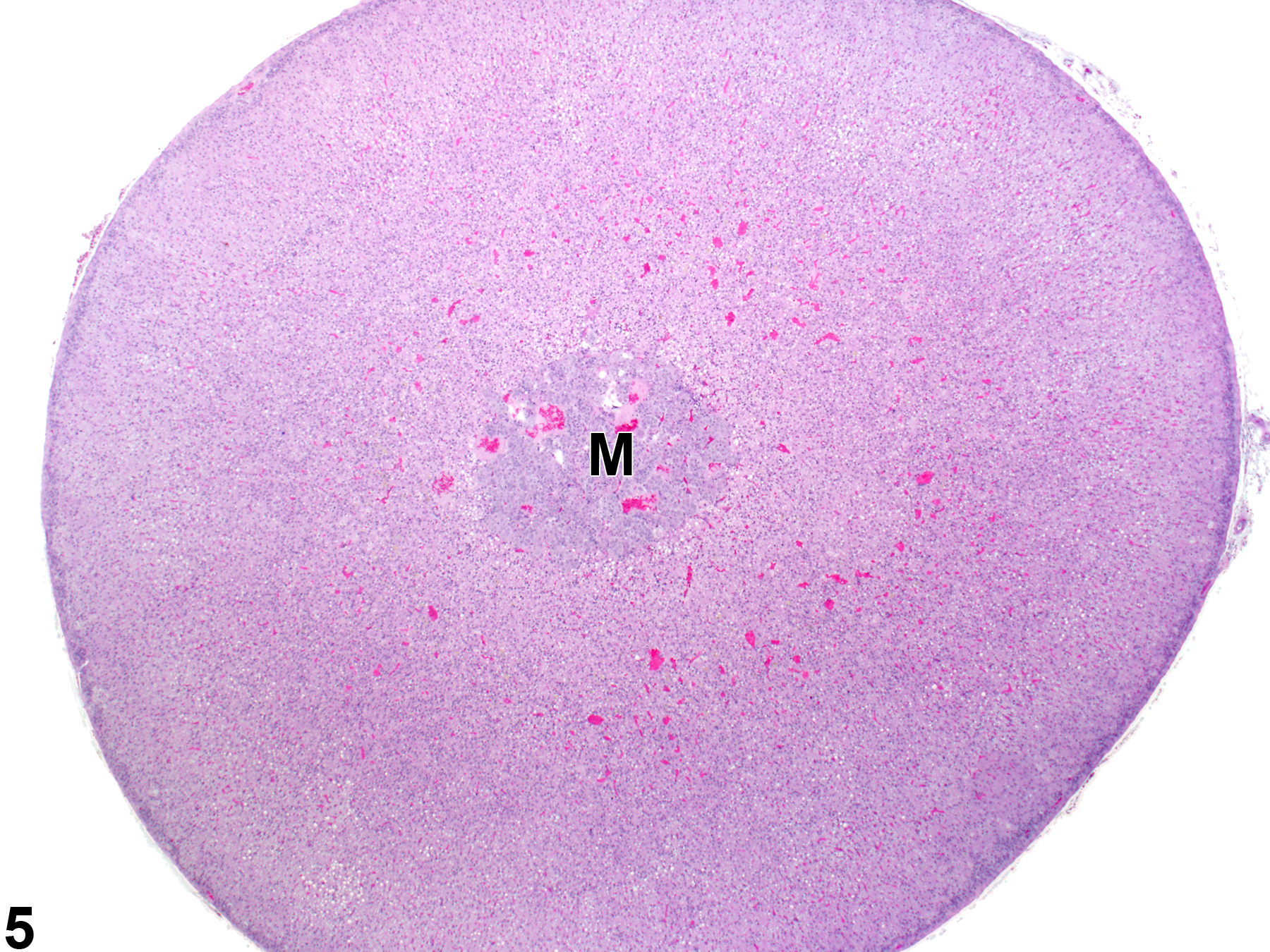
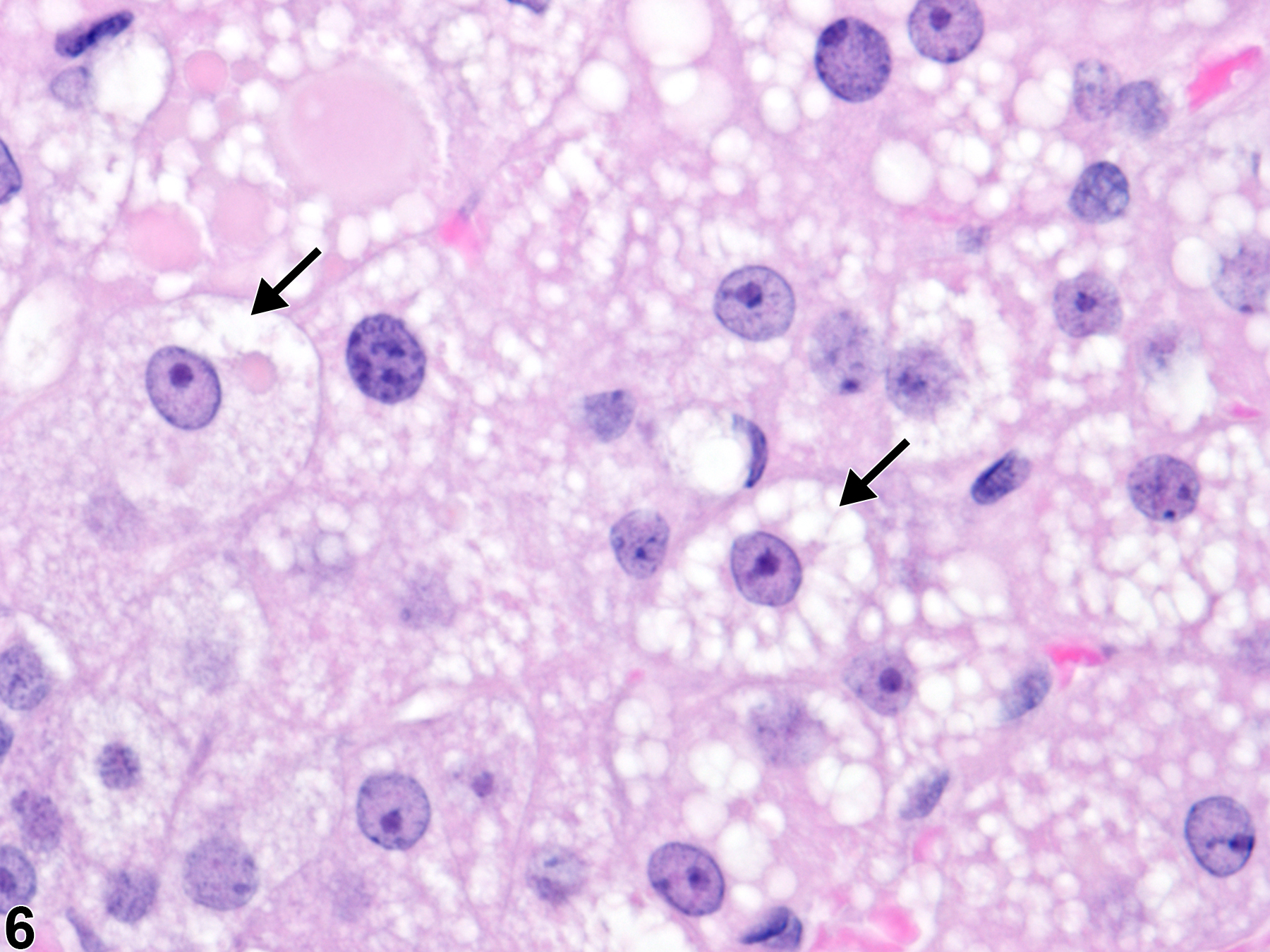
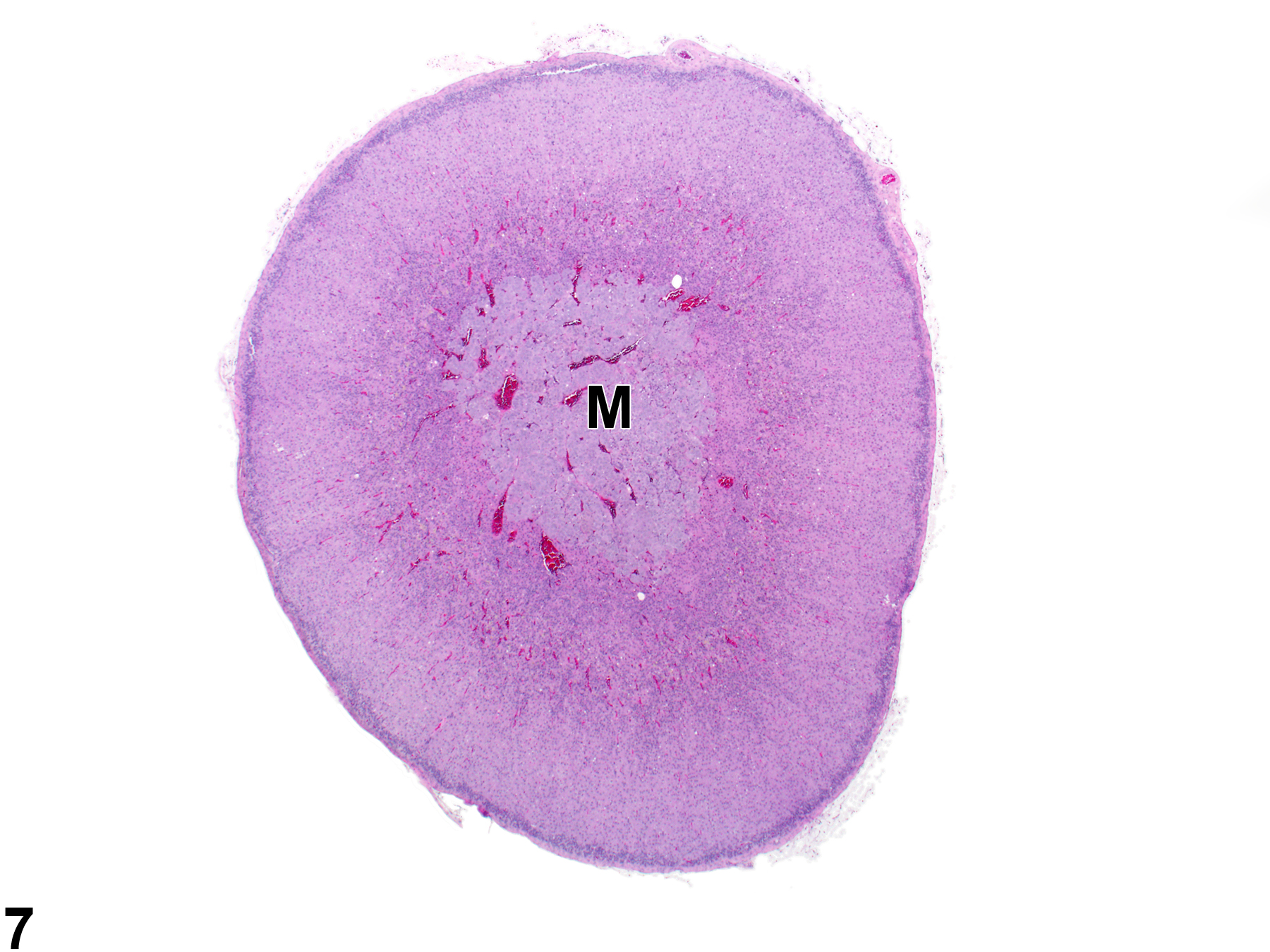
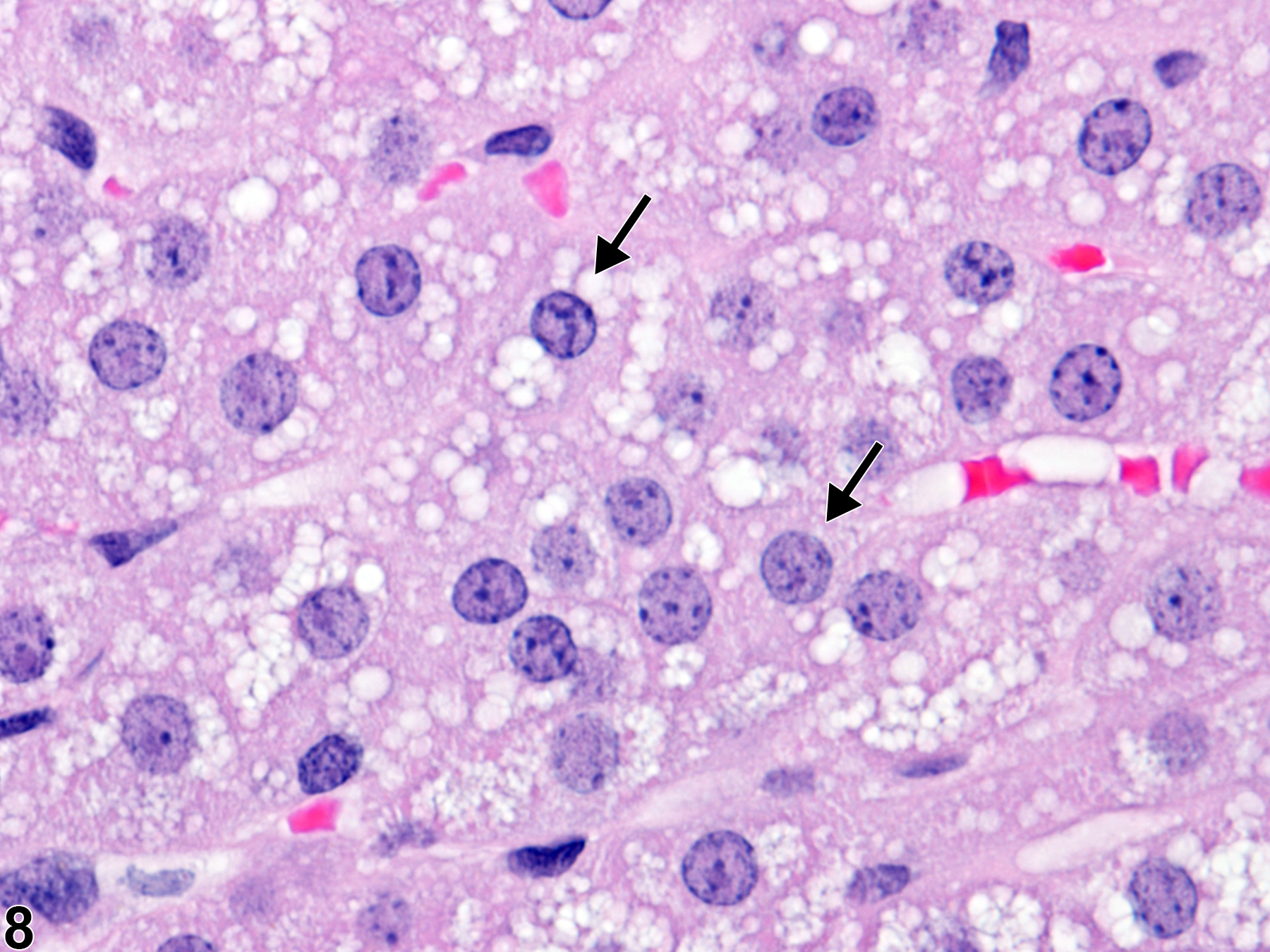
Diffuse cortical hypertrophy (Figure 5 and Figure 6) often results in pronounced widening of the cortex and overall gland enlargement compared with unaffected normal adrenal glands (Figure 7 and Figure 8).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cortical hypertrophy (of the zona fasciculata) in rats and mice usually results from elevated levels of adrenocorticotropic hormone (ACTH), which in turn can be elevated due to various causes, such as primary hypothalamic or pituitary disease or decreased glucocorticoid feedback regulation caused by adrenal cortical toxic or degenerative lesions. Diffuse, bilateral, and often prominent hypertrophy in the zona fasciculata can also be a sequela to stress from various causes, a finding that is especially common in rats.
Hypertrophy (and hyperplasia) of zona glomerulosa cells can result from derangements of the renin-angiotensin system that result in elevated angiotensin II.
Whether focal or diffuse, cortical hypertrophy is generally not considered to be a preneoplastic change. However, cortical hypertrophy (increased cell size) and hyperplasia (increased cell numbers) can often be concurrent lesions in the same gland or even in the same focus. Thus, as a practical matter, determining which change is predominant in a given lesion and/or gland can be very difficult. Cortical hypertrophy can also be confused with the cortical cell enlargement that occurs in many cases of cytoplasmic vacuolization.
Brix AE, Nyska A, Haseman JK, Sells DM, Jokinen MO, Walker NJ. 2005. Incidences of selected lesions in control female Harlan Sprague-Dawley rats from two-year studies performed by the National Toxicology Program. Toxicol Pathol 33:477-483.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/16036865Dunn TB. 1970. Normal and pathologic anatomy of the adrenal gland of the mouse, including neoplasms. J Natl Cancer Inst 44:1323-1389.
Abstract: http://jnci.oxfordjournals.org/content/44/6/1323.abstractFerreira JC, Cruz CD, Neves D, Pignatelli D. 2007. Increased extracellular signal regulated kinases phosphorylation in the adrenal gland in response to chronic ACTH treatment. J Endocrinol 192:647-658.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/17332532Frith CH, Botts S, Jokinen MP, Eighmy JJ, Hailey JR, Morgan SJ, Chandra M. 2000. Non-proliferative lesions of the endocrine system in rats, E-1. In: Guides for Toxicologic Pathology. STP/ARP/AFIP, Washington, DC.
Full Text: https://www.toxpath.org/docs/SSNDC/EndocrineNonprolifRat.pdfHamlin MH, Banas DA. 1990. Adrenal gland. In: Pathology of the Fischer Rat: Reference and Atlas (Boorman GA, Eustis SL, Elwell MR, Montgomery CA, MacKenzie WF, eds). Academic Press, San Diego, 501-518.
Abstract: https://www.ncbi.nlm.nih.gov/nlmcatalog/9002563Harvey PW, Sutcliffe C. 2010. Adrenocortical hypertrophy: Establishing cause and toxicological significance. J Appl Toxicol 30:617-626.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/20687119Mazzocchi G, Rebuffat P, Belloni AS, Robba C, Nussdorfer GG. 1980. An ultrastructural stereologic study of the effects of angiotensin II on the zona glomerulosa of the rat adrenal cortex. Acta Endocrinol 95:523-527.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/7006292McEwan PE, Lindop GB, Kenyon CJ. 1996. Control of cell proliferation in the rat adrenal gland in vivo by the renin-angiotensin system. Am J Physiol (Endocrinol Metab) 34:E192-E198.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/8760097National Toxicology Program. 2006. NTP TR-520. Toxicology and Carcinogenesis Studies of 3,3',4,4',5-Pentachlorobiphenyl (PCB 126) (CAS No. 57465-28-8) in Female Harlan Sprague-Dawley Rats (Gavage Studies). NTP, Research Triangle Park, NC.
Abstract: https://ntp.niehs.nih.gov/go/9301National Toxicology Program. 2013. NTP TR-578. Toxicology and Carcinogenesis Studies of Gingko biloba Extract in F344/N Rats and B6C3F1 Mice (Gavage Studies). NTP, Research Triangle Park, NC.
Abstract: https://ntp.niehs.nih.gov/go/37193Nyska A, Maronpot RR. 1990. Adrenal gland. In: Pathology of the Mouse: Reference and Atlas (Maronpot RR, Boorman GA, Gaul BW, eds). Cache River Press, Vienna, IL, 509-536.
Ulrich-Lai YM, Figueiredo HF, Ostrander MM, Choi DC, Engeland WC, Herman JP. 2006. Chronic stress induces adrenal hyperplasia and hypertrophy in a subregion-specific manner. Am J Physiol (Endocrinol Metab) 291:E965-E973.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/16772325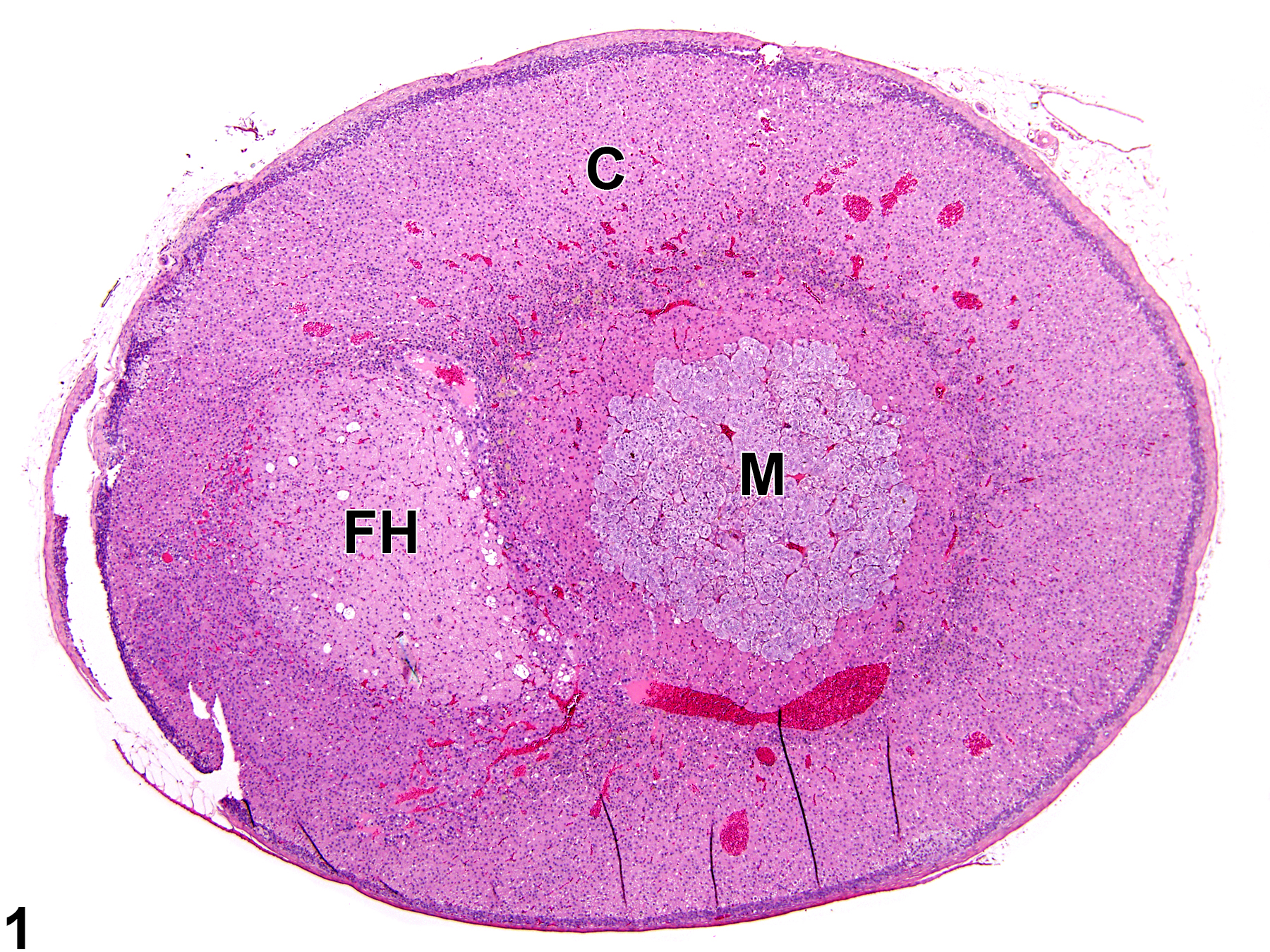
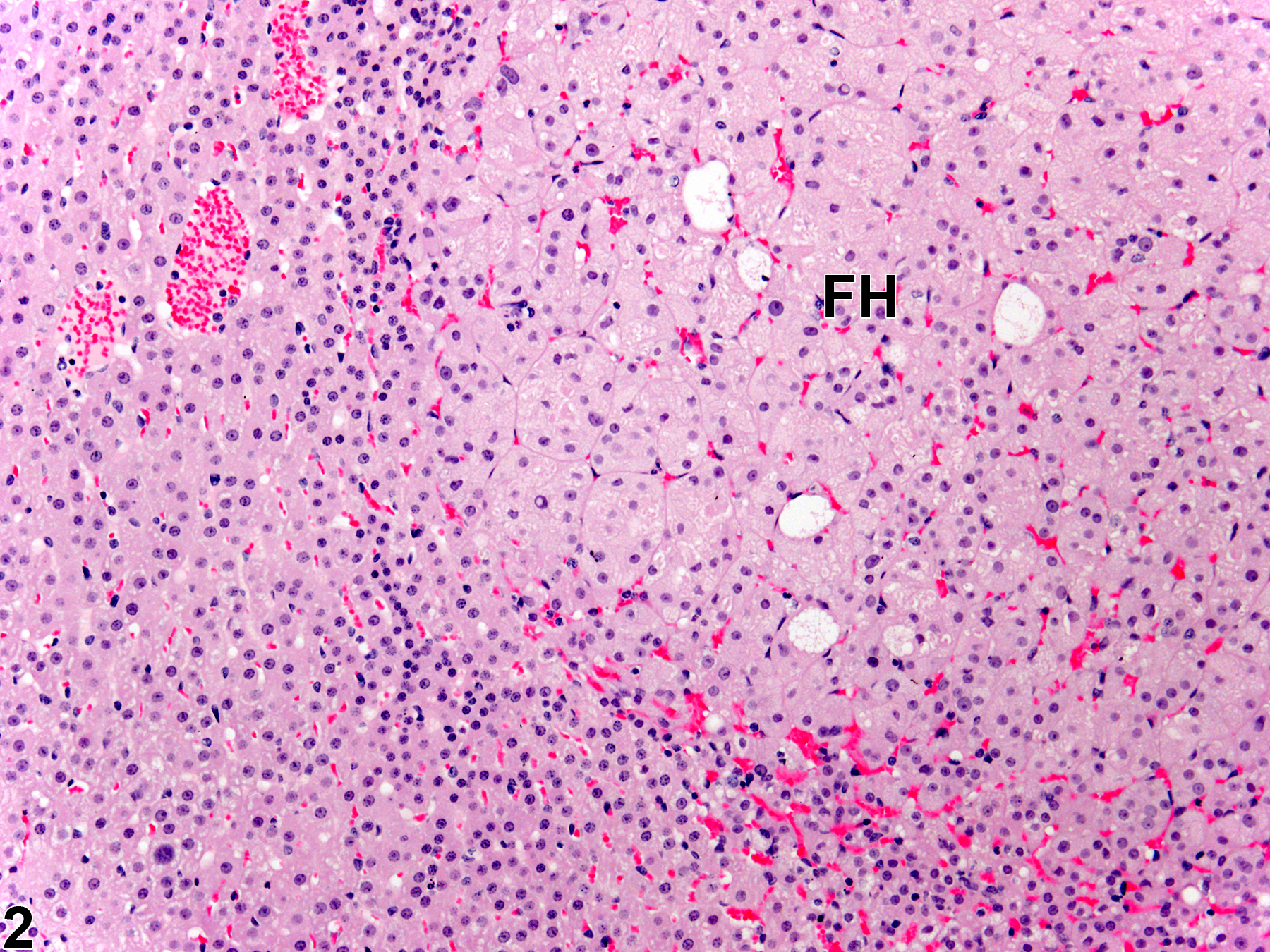
Adrenal gland, Cortex - Hypertrophy in a female Sprague-Dawley rat from a chronic study. There is a well-demarcated, noncompressive focal area in which the cells are enlarged (FH). C = cortex, M = medulla.
All Images

Adrenal gland, Cortex - Hypertrophy in a female Sprague-Dawley rat from a chronic study. There is a well-demarcated, noncompressive focal area in which the cells are enlarged (FH). C = cortex, M = medulla.

Adrenal gland, Cortex - Hypertrophy in a female Sprague-Dawley rat from a chronic study (higher magnification of Figure 1). The cells in this focus of hypertrophy (FH) have increased amounts of pale eosinophilic cytoplasm.

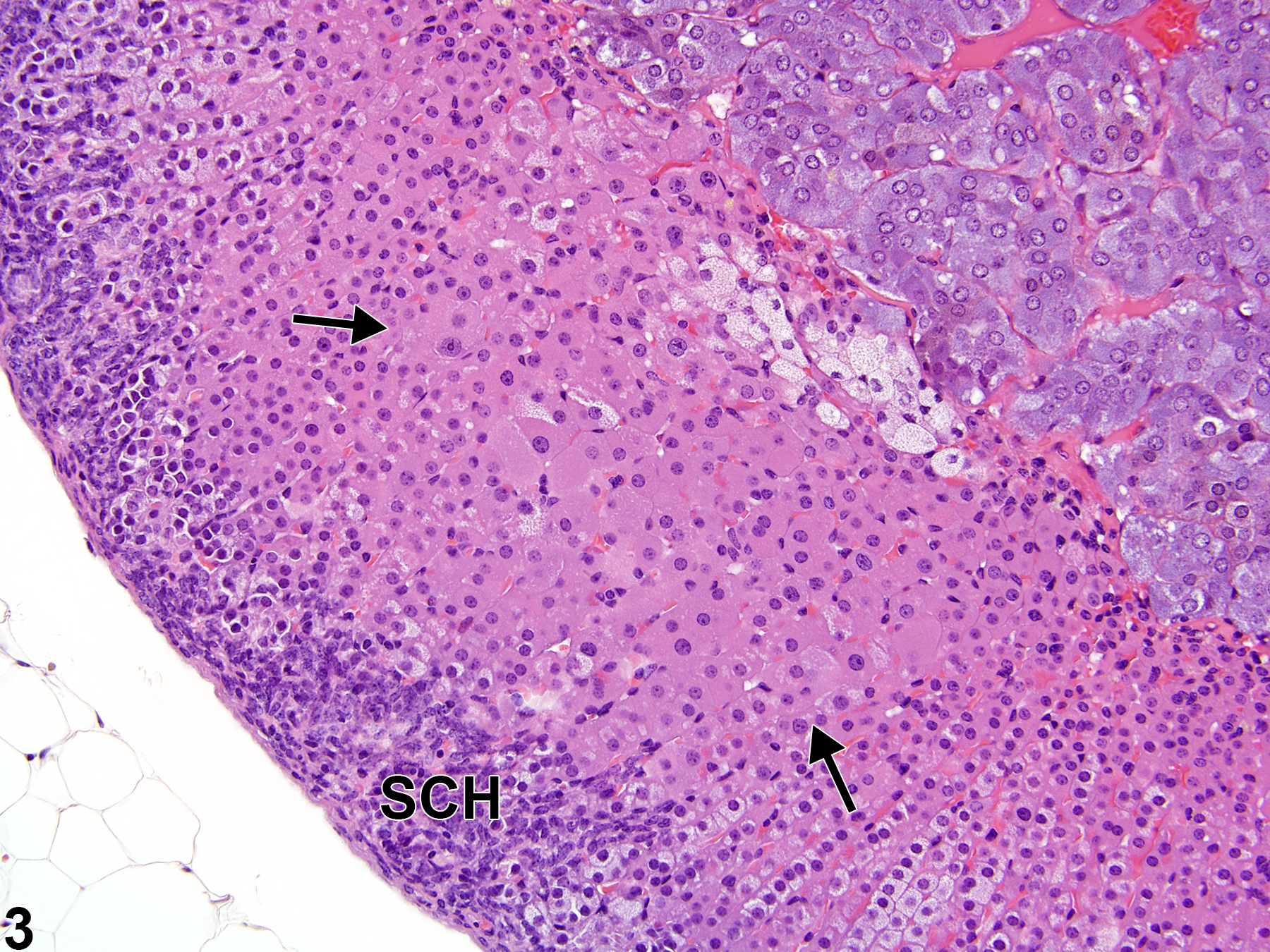
Adrenal gland, Cortex - Hypertrophy in a male B6C3F1/N/N mouse from a chronic study. There is a focus of enlarged cells (arrows) in the cortex that slightly compresses the adjacent parenchyma; there is also subcapsular hyperplasia (SCH).

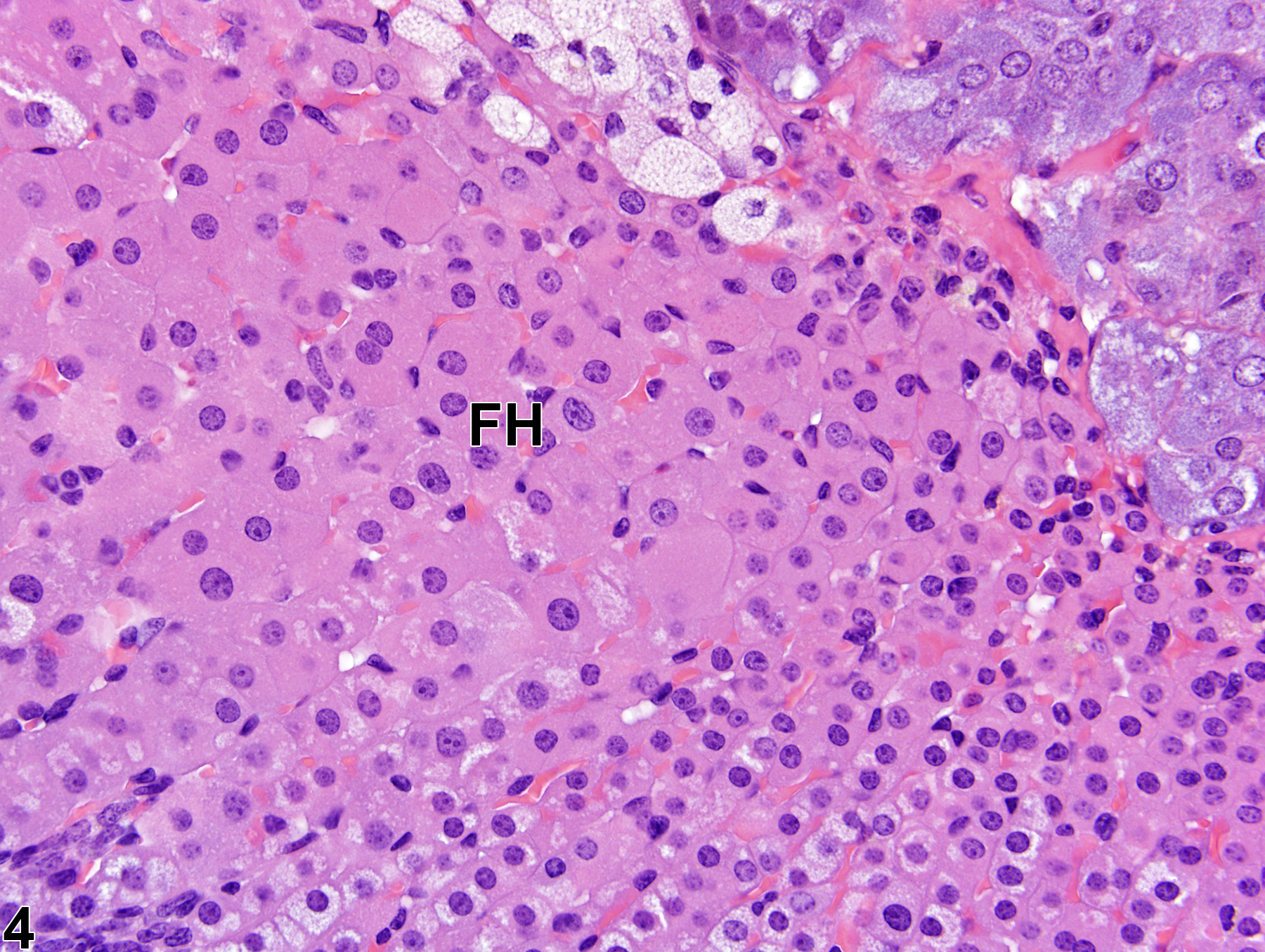
Adrenal gland, Cortex - Hypertrophy in a male B6C3F1/N/N mouse from a chronic study (higher magnification of Figure 3). The cells in this focus of hypertrophy (FH) have increased amounts of pale eosinophilic cytoplasm and slightly enlarged nuclei.

Adrenal gland, Cortex - Hypertrophy in a male F344/N rat from a chronic study. Diffuse cortical hypertrophy results in pronounced overall gland enlargement. M = medulla.

Adrenal gland, Cortex - Hypertrophy in a male F344/N rat from a chronic study (higher magnification of Figure 5). The hypertrophic cortical cells (arrows) have increased cytoplasmic volume.

Adrenal gland, Cortex - Normal in a male F344/N rat from a chronic study. A normal adrenal gland at the same magnification as Figure 5 6 is shown for comparison. M = medulla.

Adrenal gland, Cortex - Normal in a male F344/N rat from a chronic study. A normal adrenal gland at the same magnification as Figure 6 is shown for comparison.