

Endocrine System
Thyroid Gland - Inflammation
Narrative
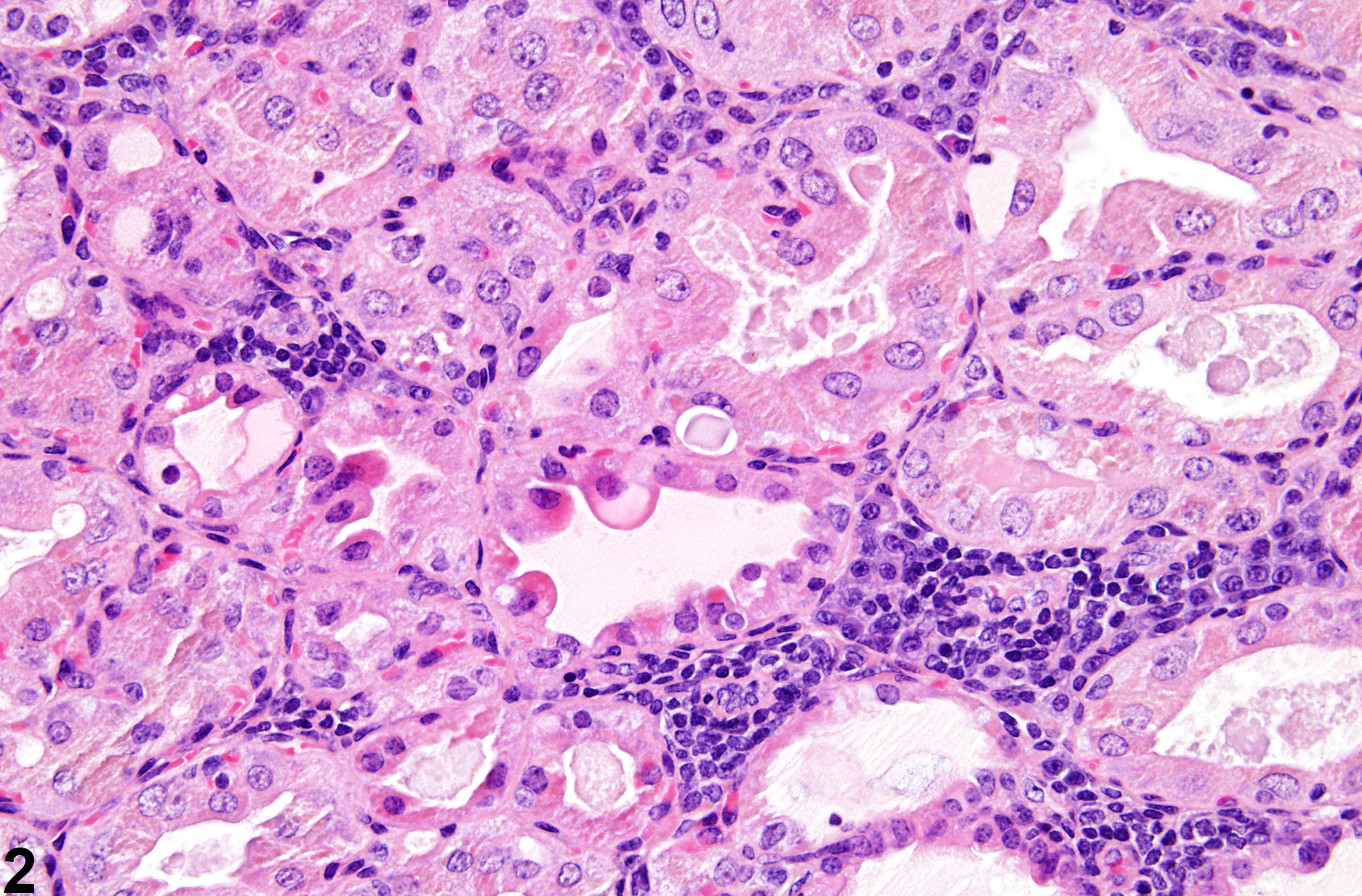
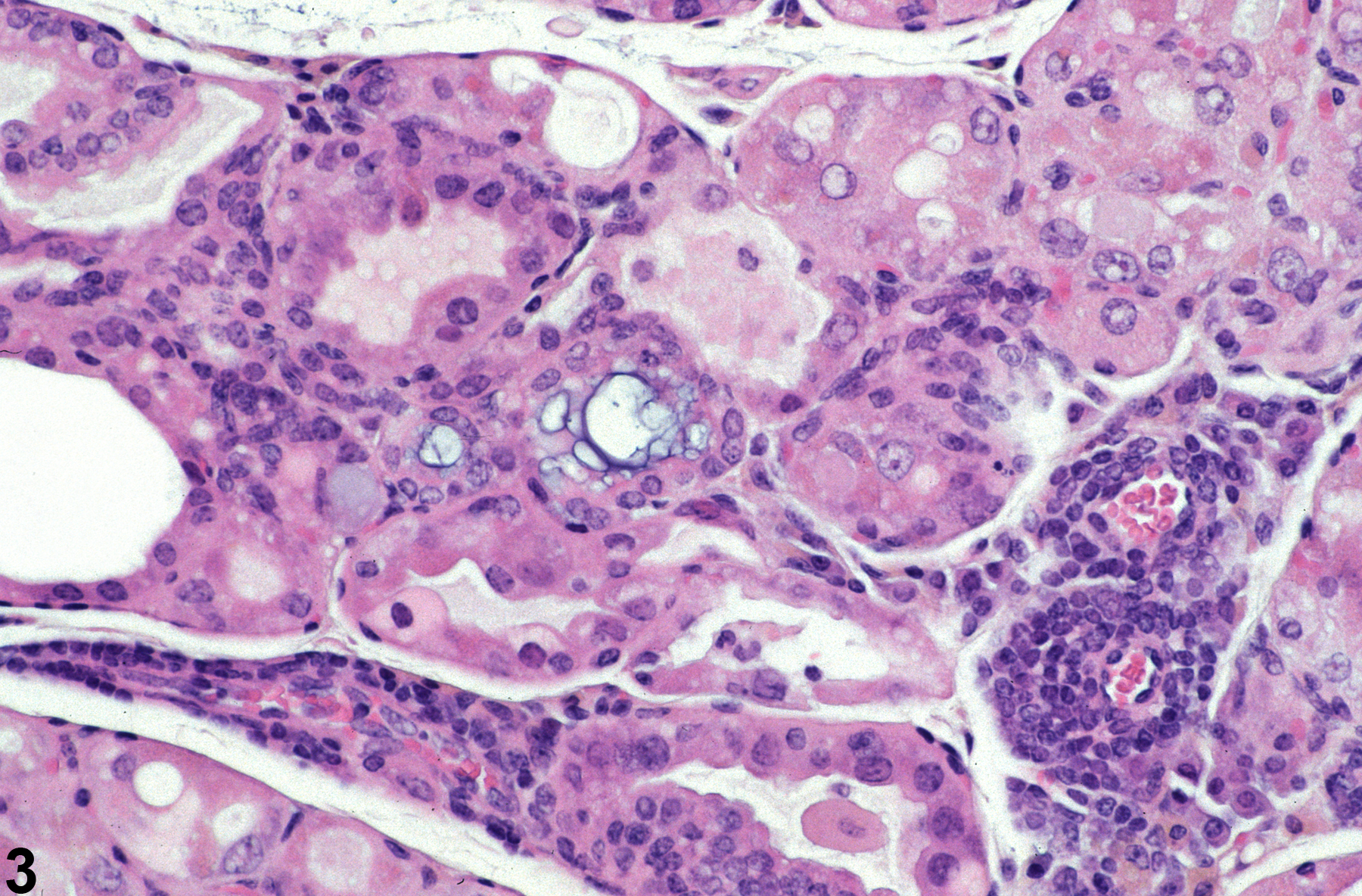
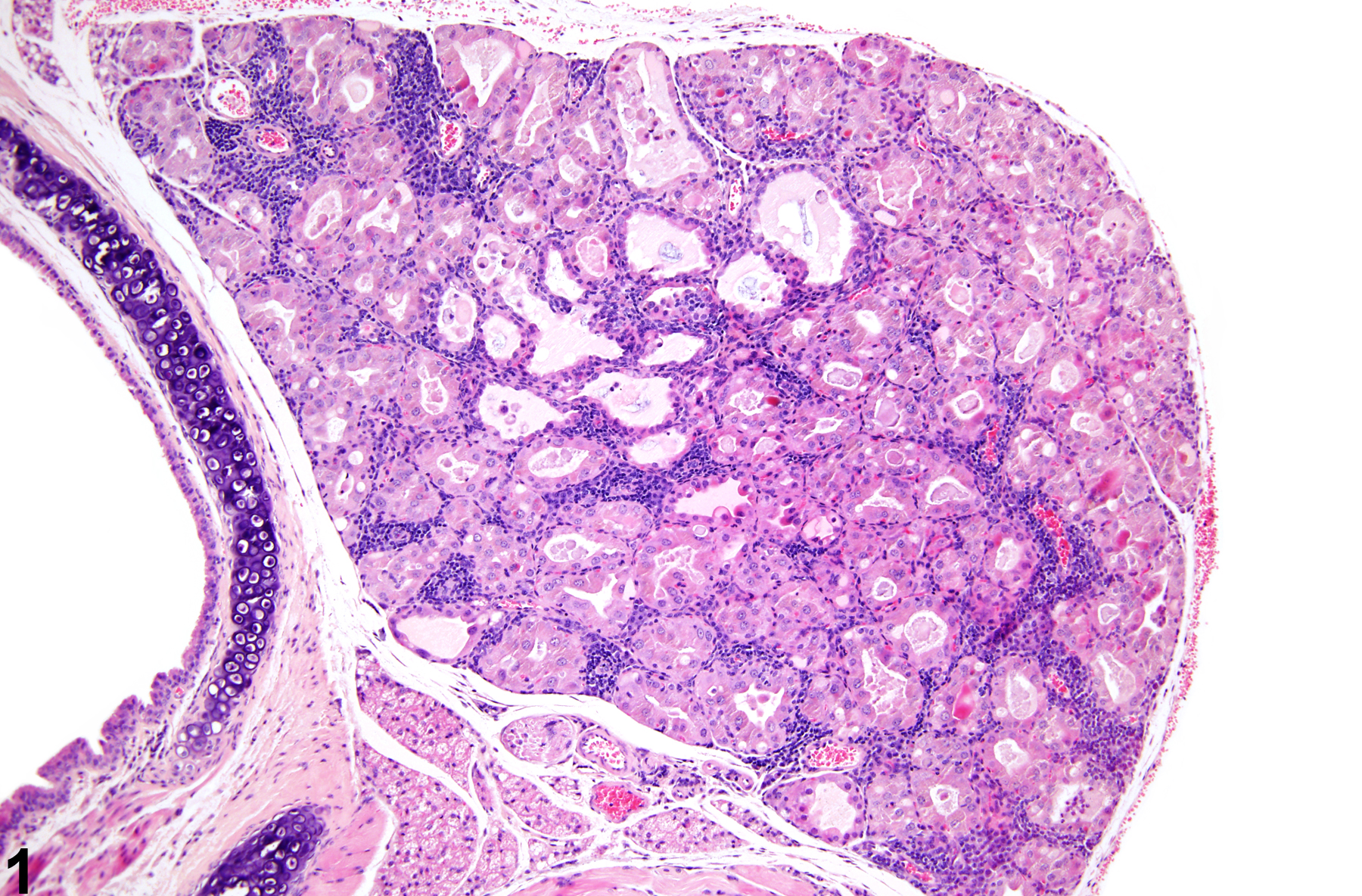
Spontaneously occurring cellular infiltrates are rare in thyroid glands of mice and rats. Multiple changes are present in the thyroids of these treated mice (Figure 1, Figure 2, and Figure 3). Lymphoid cell infiltrates are present between follicles (Figure 1 and Figure 2) and in perivascular spaces (Figure 3). Additionally there is hypertrophy, degeneration, and necrosis of follicular epithelium.
{kind=link}
{kind=link}
Greaves P. 2007. Histopathology of Preclinical Toxicity Studies: Interpretation and Relevance in Drug Safety Evaluation, 3rd ed. Academic Press, Amsterdam, 819-839.
Abstract: http://www.sciencedirect.com/science/book/9780444527714Hardisty JF, Boorman GA. 1999. Thyroid and parathyroid glands. In: Pathology of the Mouse: Reference and Atlas (Maronpot RR, Boorman GA, Gaul BW, eds). Cache River Press, Vienna, IL, 537–554.
Thyroid Gland - Inflammation, chronic in a female Tg.AC (FVB/N) mouse from a subchronic study. Small aggregates of lymphoid cells are present at multiple sites between follicles.
All Images

Thyroid Gland - Inflammation, chronic in a female Tg.AC (FVB/N) mouse from a subchronic study. Small aggregates of lymphoid cells are present at multiple sites between follicles.

Thyroid Gland - Inflammation, chronic in a female Tg.AC (FVB/N) mouse from a subchronic study. Higher magnification of the small aggregates of lymphoid cells in Figure 1.

Thyroid Gland - Inflammation, chronic in a female Tg.AC (FVB/N) mouse from a subchronic study. A perivascular accumulation of lymphoid cells is present.