

Hematopoietic System
Bone Marrow - Fibrosis
Narrative
{kind=link}
{kind=link}
While it is not clear in rodent toxicity or preclinical studies if there is a need to distinguish among fibrosis types, much has been recently learned in humans regarding this topic. In humans, increased reticulin fibers are associated with many benign and malignant conditions, while increased collagen is prominent in late stages of myeloproliferative diseases or following metastasis to the bone marrow. The amount of reticulin staining in the bone marrow often has no correlation with disease severity, while increases in collagen staining are associated with more severe disease and a poorer prognosis. In addition, reticulin fibrosis is more likely to reverse than is collagen fibrosis after removal or successful treatment of the causative disorder.
Although much about the pathophysiology of (secondary) bone marrow fibrosis remains to be elucidated, it is known that cytokines from bone marrow macrophages, megakaryocytes, and platelets appear to be necessary for fibrosis to occur. These include platelet-derived growth factor and transforming growth factor-β. Additionally, fibrosis has been induced in mice injected with high amounts of recombinant thrombopoietin.
The fibroproliferative and osteosclerotic lesions of fibrous osteodystrophy and fibro-osseous lesions are well-defined lesions of rodent bone with distinct histologic characteristics (see the chapter on bone). Thus, it is inappropriate to use the term “fibrosis” to diagnose these lesions.
The diagnostic term “myelofibrosis” should not be used to describe fibrotic lesions of the bone marrow in mice and rats. In humans, myelofibrosis is an abbreviated term that has been used in reference to chronic idiopathic myelofibrosis or primary myelofibrosis. This disease is a distinct clonal myeloproliferative disease characterized by a reactive, progressive fibrosis occurring in response to a neoplastic myeloid and/or megakaryocytic proliferation and is accompanied by specific hematologic and clinical findings. Since a similar disorder has not been documented in rodents, it is best to avoid use of the term “myelofibrosis.”
Bain BJ, Clark DM, Lampert IA, Wilkins BS. 2001. Bone Marrow Pathology, 3rd ed. Blackwell, Ames, IA, 90-140.
Abstract: http://onlinelibrary.wiley.com/book/10.1002/9780470757130Kuter DJ, Bain B, Mufti G, Bagg A, Hasserjian RP. 2007. Bone marrow fibrosis: Pathophysiology and clinical significance of increased bone marrow stromal fibres. Br J Haematol 139:351-362.
Abstract: http://www.ncbi.nlm.nih.gov/pubmed/17910625MacKenzie WF, Eustis SL. 1990. Bone marrow. In: Pathology of the Fischer Rat: Reference and Atlas (Boorman GA, Eustis SL, Elwell MR, Montgomery CA, Mackenzie WF, eds). Academic Press, San Diego, 315-337.
Abstract: http://www.ncbi.nlm.nih.gov/nlmcatalog/9002563Travlos GS. 2006. Histopathology of the bone marrow. Toxicol Pathol 34:566-598.
Abstract: http://tpx.sagepub.com/content/34/5/566.abstractWeiss DJ. 2010. Chronic inflammation and secondary myelofibrosis. In: Schalm’s Veterinary Hematology, 5th ed (Weiss DJ, Wardrop KJ, eds). Wiley-Blackwell, Ames, IA, 112-117.
Abstract: http://vet.sagepub.com/content/40/2/223.1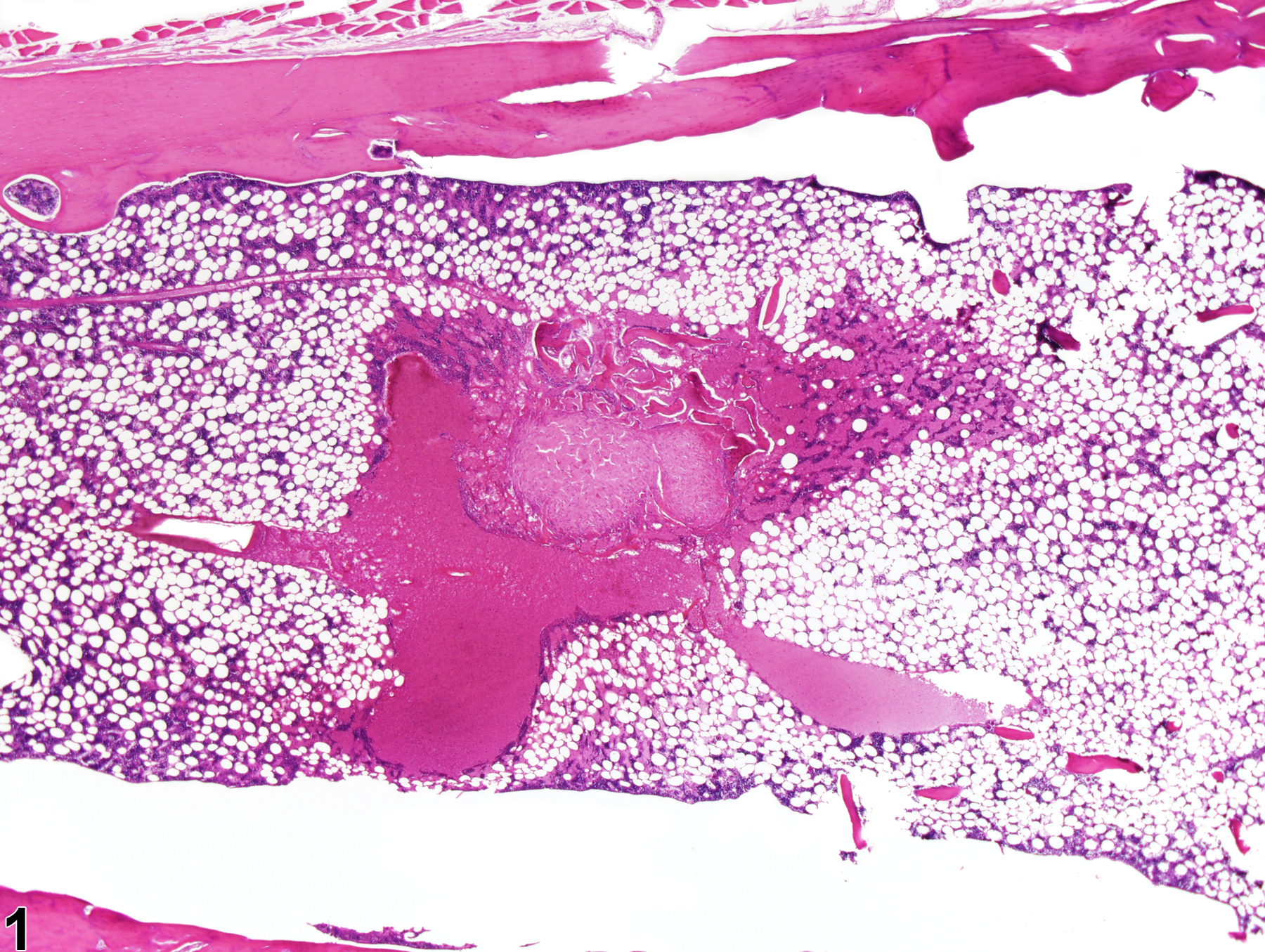
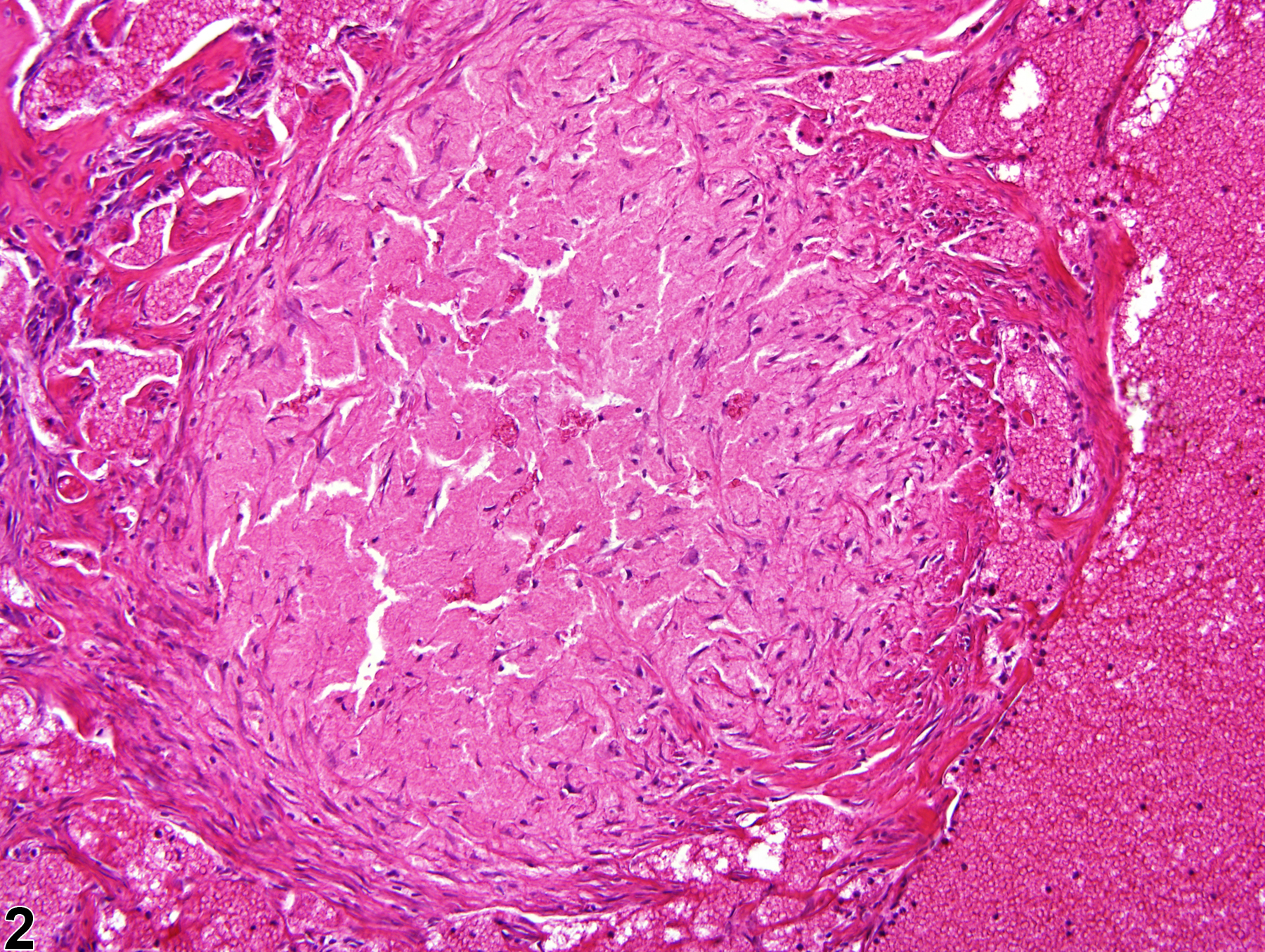
Dense fibrous tissue surrounded by areas of angiectasis is present in bone marrow in a male F344/N rat from a chronic study.
All Images

Dense fibrous tissue surrounded by areas of angiectasis is present in bone marrow in a male F344/N rat from a chronic study.

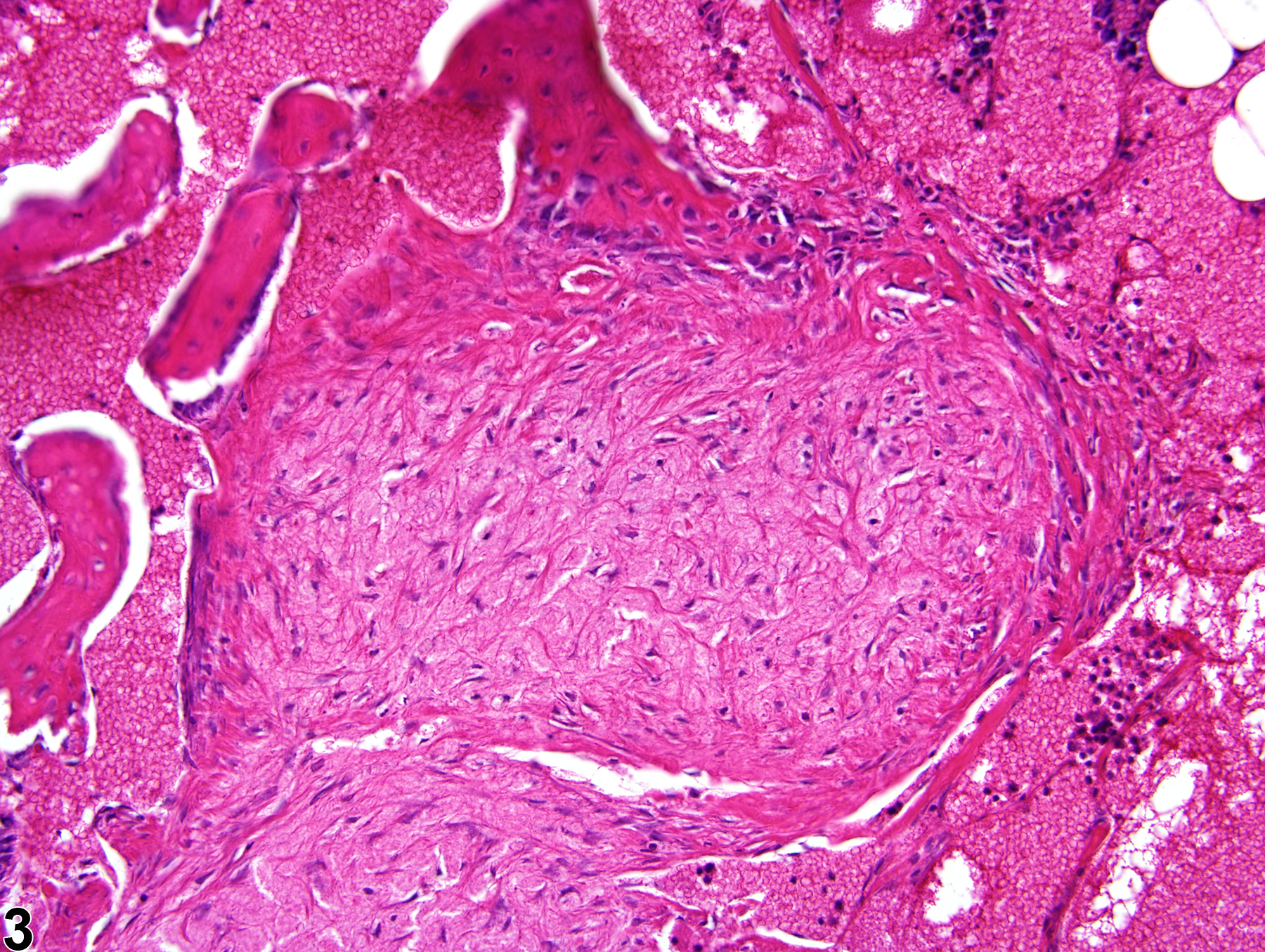
Higher magnification of Figure 1 showing dense fibrous tissue surrounded by areas of angiectasis in bone marrow in a male F344/N rat from a chronic study.

Higher magnification of Figure 1 showing dense fibrous tissue surrounded by areas of angiectasis in bone marrow in a male F344/N rat from a chronic study.