

Reproductive System, Male
Testis - Inflammation
Narrative
Comment:
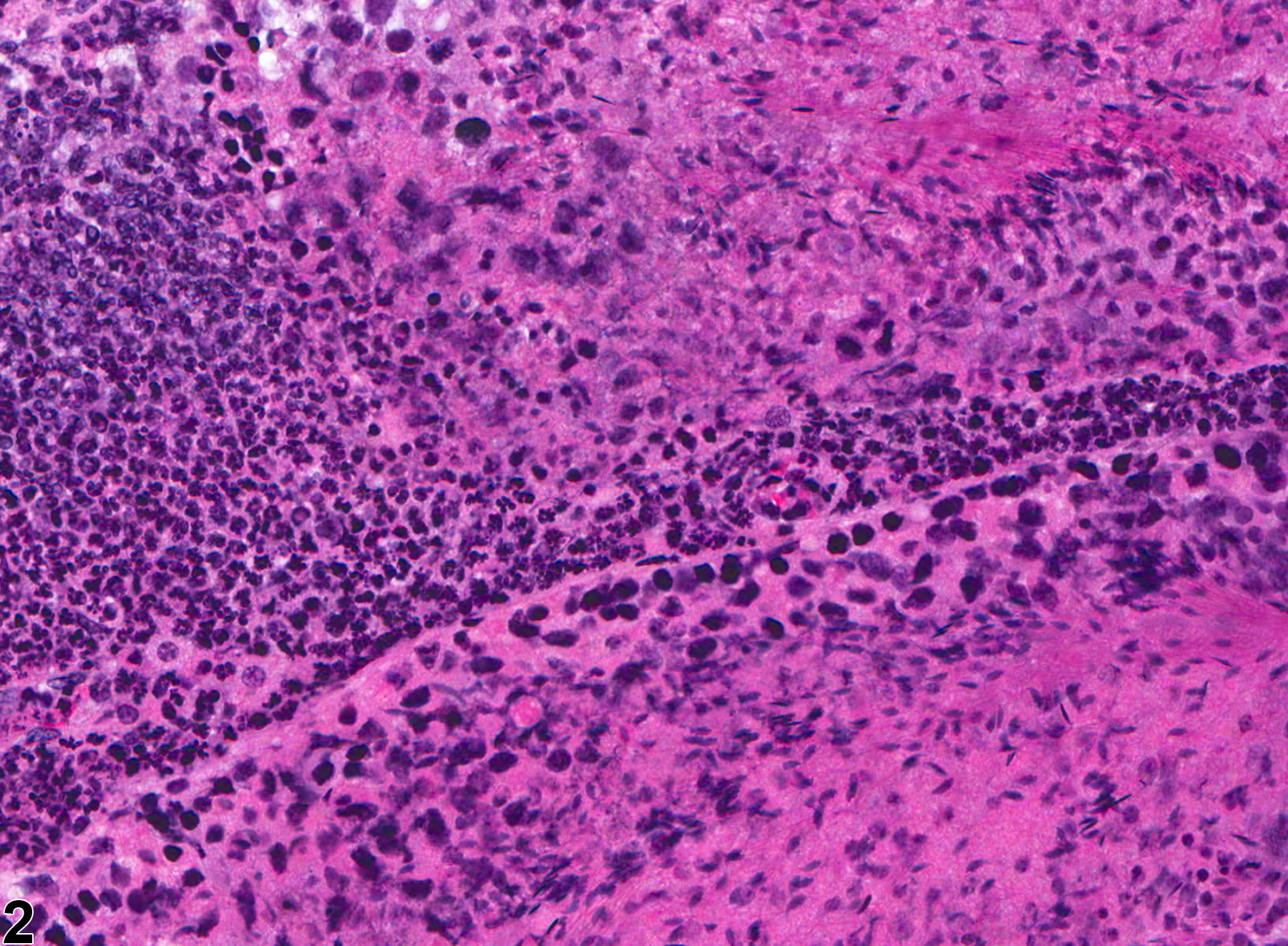
Testicular inflammation is characterized by infiltration of inflammatory cells in response to tissue damage. Inflammatory responses in the testis are very uncommon and are usually seen only in response to seminiferous tubular necrosis or tissue damage sufficient to break down the Sertoli cell tight junctions that make up the blood-testis barrier. Seminiferous tubular degeneration and atrophy are generally not accompanied by an inflammatory response. Inflammatory infiltrates are rarely seen as a direct response to chemical agents; an exception is the acute response to the Sertoli cell toxicant di-n-pentyl phthalate, where a transient, interstitial neutrophilic infiltrate occurred and was associated with the release of interleukin prior to any significant tubular damage. In most cases the inflammatory infiltrate remains in the interstitial compartment, but it may penetrate the seminiferous tubules and, rarely, destroy and replace them with fibrosis. The cellular exudate determines the type of inflammation, which is predominantly neutrophilic in the example shown in Figure 1 and Figure 2 but may also be lymphocytic or granulomatous. Testicular inflammation can be unilateral or bilateral.
NTP studies have five standard categories of inflammation: acute, suppurative, chronic, chronic-active, and granulomatous. In acute inflammation, the predominant infiltrating cell is the neutrophil, thoughfewer macrophages and lymphocytes may also be present. There may also be evidence of edema orhyperemia. The neutrophil is also the predominant infiltrating cell type in suppurative inflammation, but they are aggregated, and many of them are degenerate (suppurative exudate). Cell debris from both the resident cell populations and infiltrating leukocytes, proteinaceous fluid containing fibrin, fewer macrophages, occasional lymphocytes or plasma cells, and, possibly, an infectious agent may also be present within the exudate. Grossly, these lesions would be characterized by the presence of pus. The tissue surrounding the exudate may have fibroblasts, fibrous connective tissue, and mixed inflammatory cells, depending on the chronicity of the lesion. Lymphocytes predominate in chronic inflammation. Lymphocytes also predominate in chronic-active inflammation, but there are also a significant number of neutrophils. Both lesions may contain macrophages. Granulomatous inflammation is another form of chronic inflammation, but this diagnosis requires the presence of a significant number of aggregated, large, activated macrophages, epithelioid macrophages, or multinucleated giant cells.
{kind=link}
NTP studies have five standard categories of inflammation: acute, suppurative, chronic, chronic-active, and granulomatous. In acute inflammation, the predominant infiltrating cell is the neutrophil, thoughfewer macrophages and lymphocytes may also be present. There may also be evidence of edema orhyperemia. The neutrophil is also the predominant infiltrating cell type in suppurative inflammation, but they are aggregated, and many of them are degenerate (suppurative exudate). Cell debris from both the resident cell populations and infiltrating leukocytes, proteinaceous fluid containing fibrin, fewer macrophages, occasional lymphocytes or plasma cells, and, possibly, an infectious agent may also be present within the exudate. Grossly, these lesions would be characterized by the presence of pus. The tissue surrounding the exudate may have fibroblasts, fibrous connective tissue, and mixed inflammatory cells, depending on the chronicity of the lesion. Lymphocytes predominate in chronic inflammation. Lymphocytes also predominate in chronic-active inflammation, but there are also a significant number of neutrophils. Both lesions may contain macrophages. Granulomatous inflammation is another form of chronic inflammation, but this diagnosis requires the presence of a significant number of aggregated, large, activated macrophages, epithelioid macrophages, or multinucleated giant cells.
Recommendations:
Whenever present, inflammation should be recorded, classified, graded, and described in the pathology narrative, if exacerbated by treatment. If both testes are affected, the diagnosis should be qualified as bilateral and the severity based on the more severely affected testis.
References:
Creasy DM, Foster JR, Foster PM. 1983. The morphological development of di-n-pentyl phthalate induced testicular atrophy in the rat. J Pathol 139:309-321.
Abstract: http://www.ncbi.nlm.nih.gov/pubmed/6834175Granholm T, Creasy DM, Pöllänen P, Söder O. 1992. Di-n-pentyl phthalate-induced inflammatory changes in the rat testis are accompanied by local production of a novel lymphocyte activating factor. J Reprod Immunol 21:1-14.
Abstract: http://www.ncbi.nlm.nih.gov/pubmed/1734074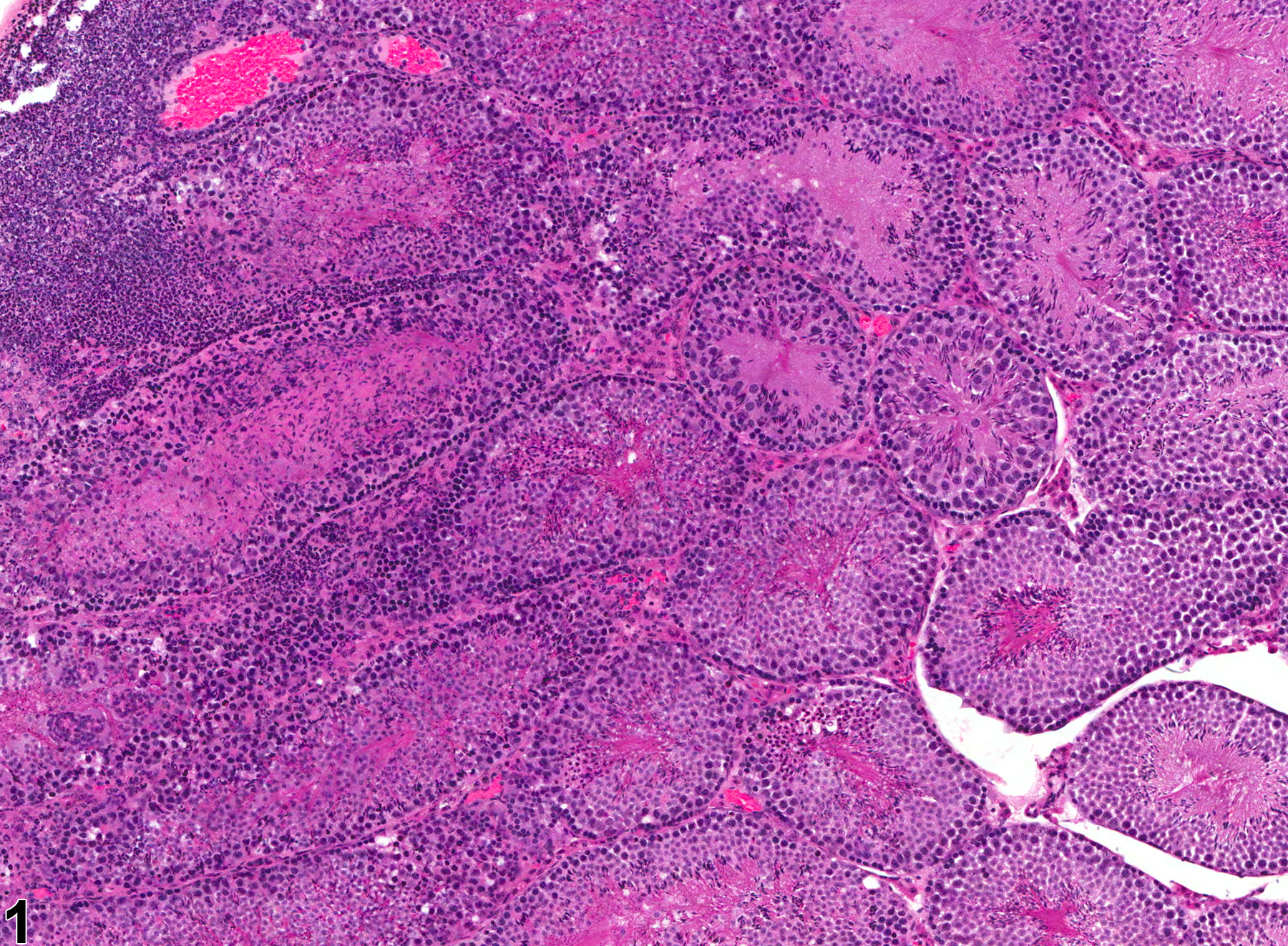
Testis - Inflammation in a male B6C3F1 mouse from a chronic study. Acute inflammation of the testis.
All Images

Testis - Inflammation in a male B6C3F1 mouse from a chronic study. Acute inflammation of the testis.

Testis - Inflammation in a male B6C3F1 mouse from a chronic study. Acute inflammation of the testis; the inflammatory cells are primarily neutrophils.