

Respiratory System
Lung, Epithelium, Alveolus - Hyperplasia
Narrative
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Boorman GA, Eustis SL. 1990. Lung. In: Pathology of the Fischer Rat: Reference and Atlas (Boorman GA, Eustis SL, Elwell MR, Montgomery CA, MacKenzie WF, eds). Academic Press, San Diego, CA, 339-367.
Dixon D, Herbert RA, Sills RC, Boorman GA. 1999. Lungs, pleura, and mediastinum. In: Pathology of the Mouse: Reference and Atlas (Maronpot RR, Boorman GA, Gaul BW, eds). Cache River Press, Vienna, IL, 293-332.
Renne, R, Brix A, Harkema J, Herbert R, Kittle B, Lewis D, March T, Nagano K, Pino M, Rittinghausen S, Rosenbruch M, Tellier P, Wohrmann T. 2009. Proliferative and nonproliferative lesions of the rat and mouse respiratory tract. Toxicol Pathol 37(suppl):5S-73S.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/20032296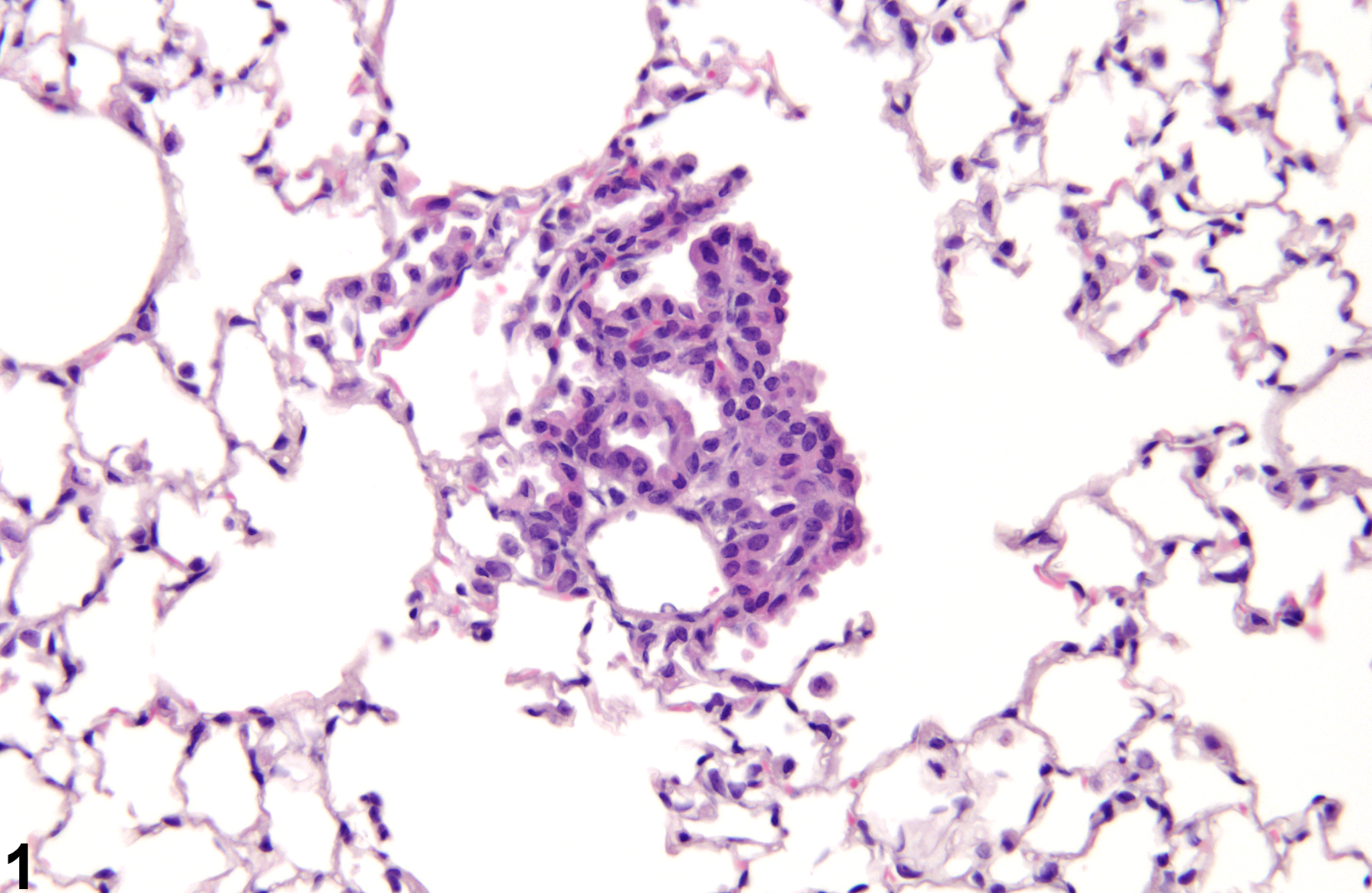
Lung, Epithelium, Alveolus - Hyperplasia in a male B6C3F1/N mouse from a chronic study. There is a small proliferation of alveolar epithelial cells with no inflammation.
All Images

Lung, Epithelium, Alveolus - Hyperplasia in a male B6C3F1/N mouse from a chronic study. There is a small proliferation of alveolar epithelial cells with no inflammation.

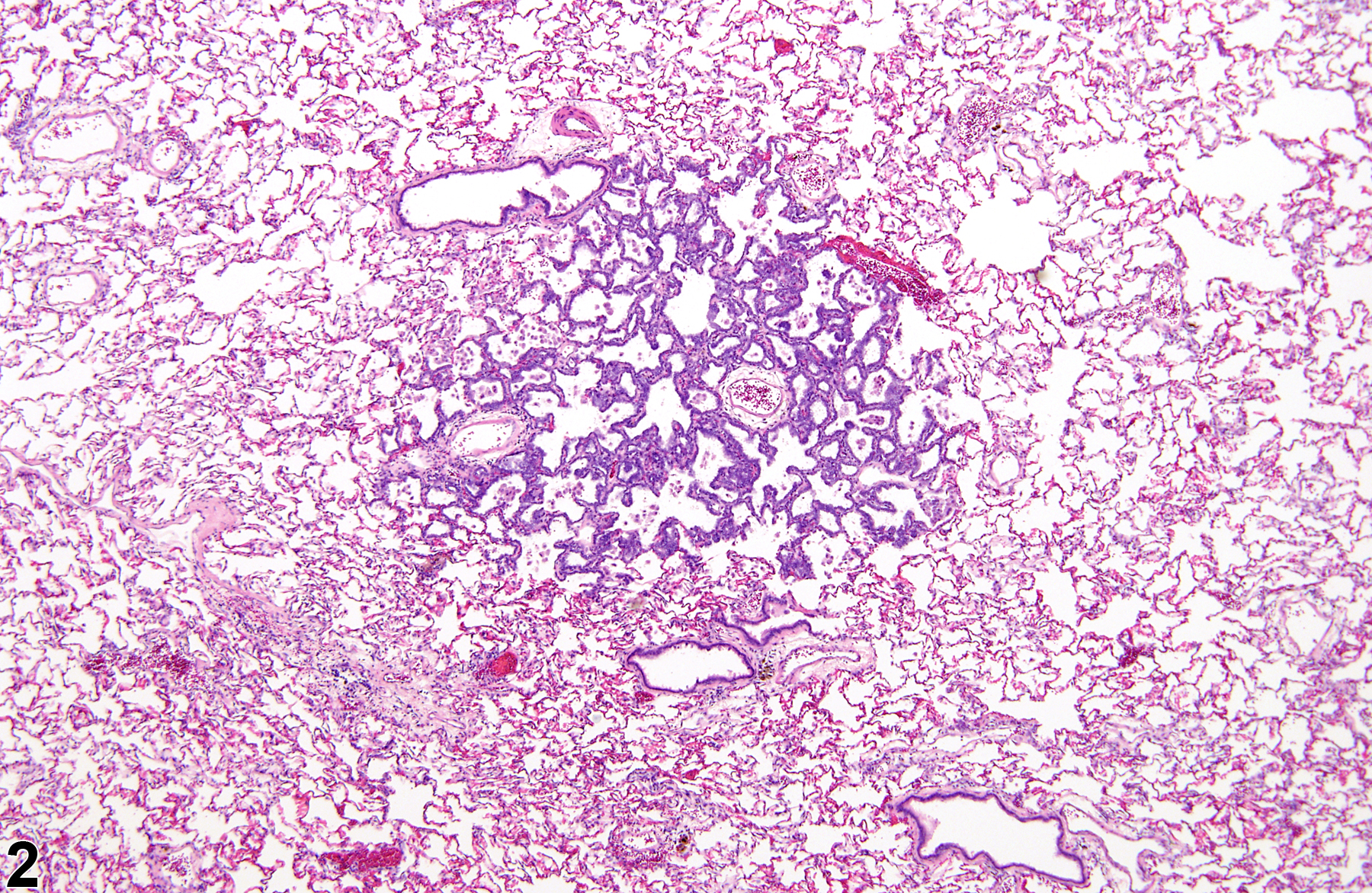
Lung, Epithelium, Alveolus - Hyperplasia in a male F344/N rat from a chronic study. There is no change in the normal alveolar architecture in this focus of alveolar epithelial hyperplasia.

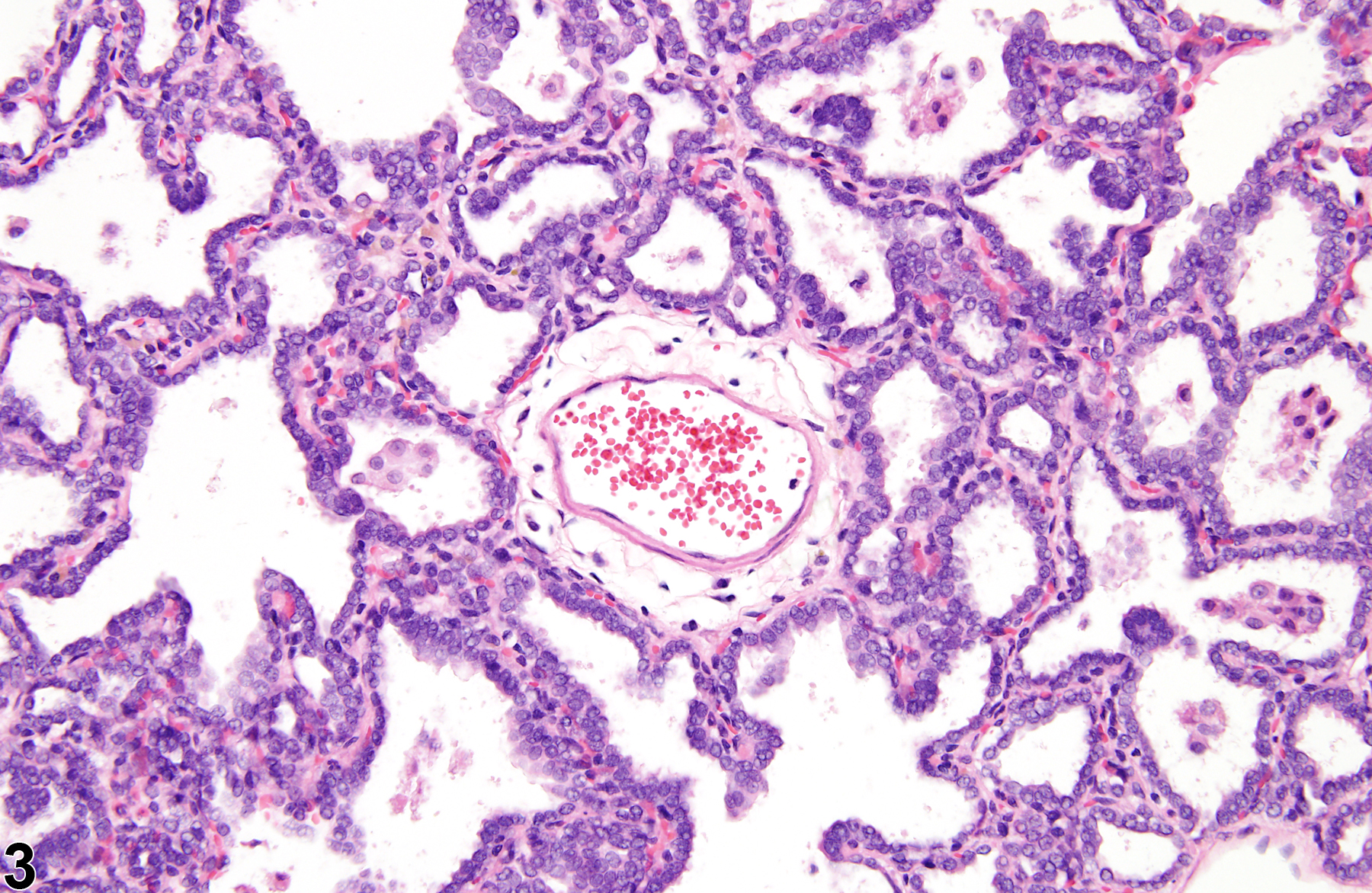
Lung, Epithelium, Alveolus - Hyperplasia in a male F344/N rat from a chronic study (higher magnification of Figure 2). The hyperplastic epithelial cells are cuboidal.

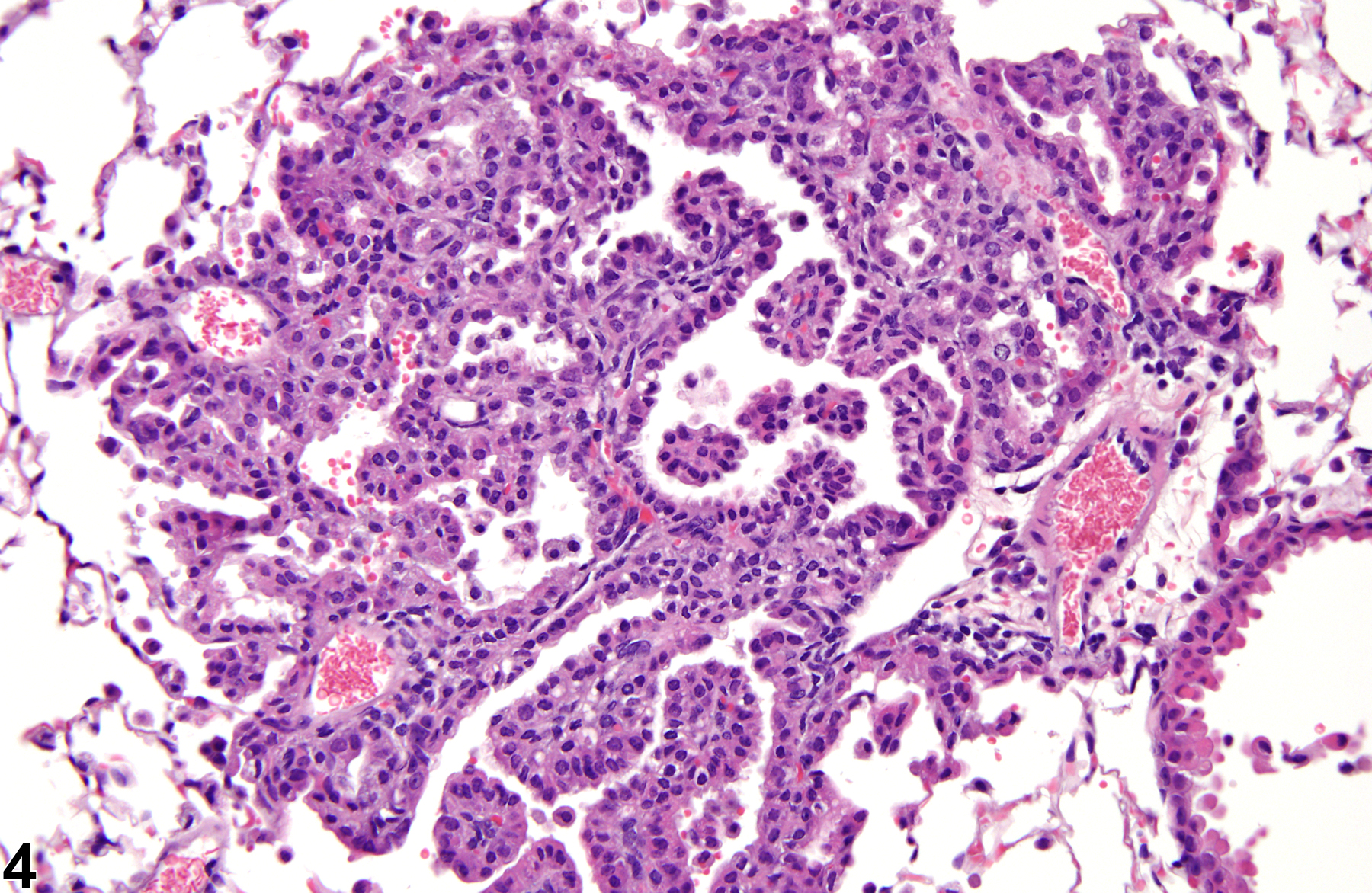
Lung, Epithelium, Alveolus - Hyperplasia in a male B6C3F1/N mouse from a chronic study. The hyperplastic epithelial cells line slightly thickened alveolar septa.

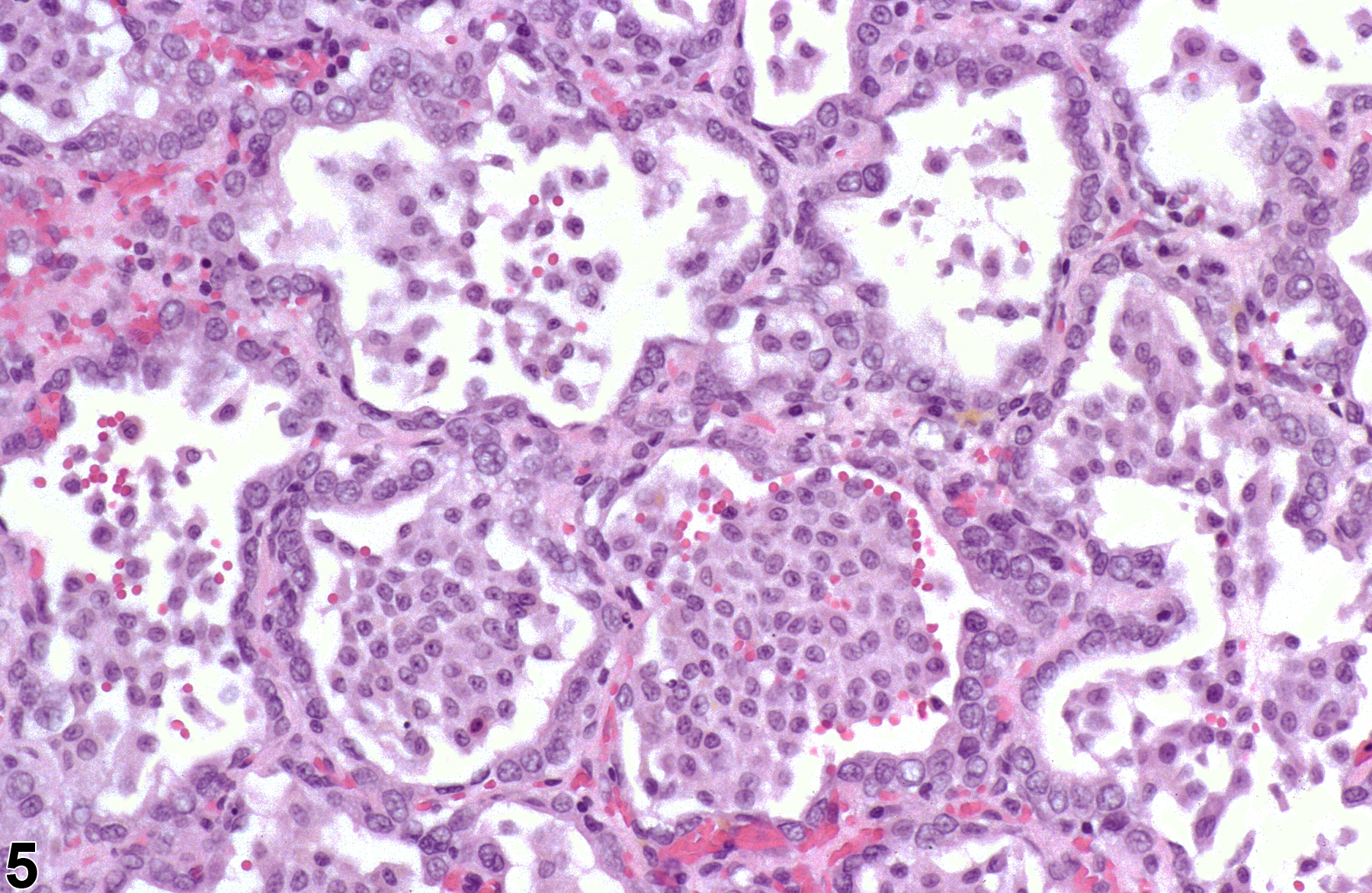
Lung, Epithelium, Alveolus - Hyperplasia in a male F344/N rat from a subchronic study. Alveolar epithelial hyperplasia secondary to inflammation is associated with numerous alveolar macrophages and minimal hemorrhage.

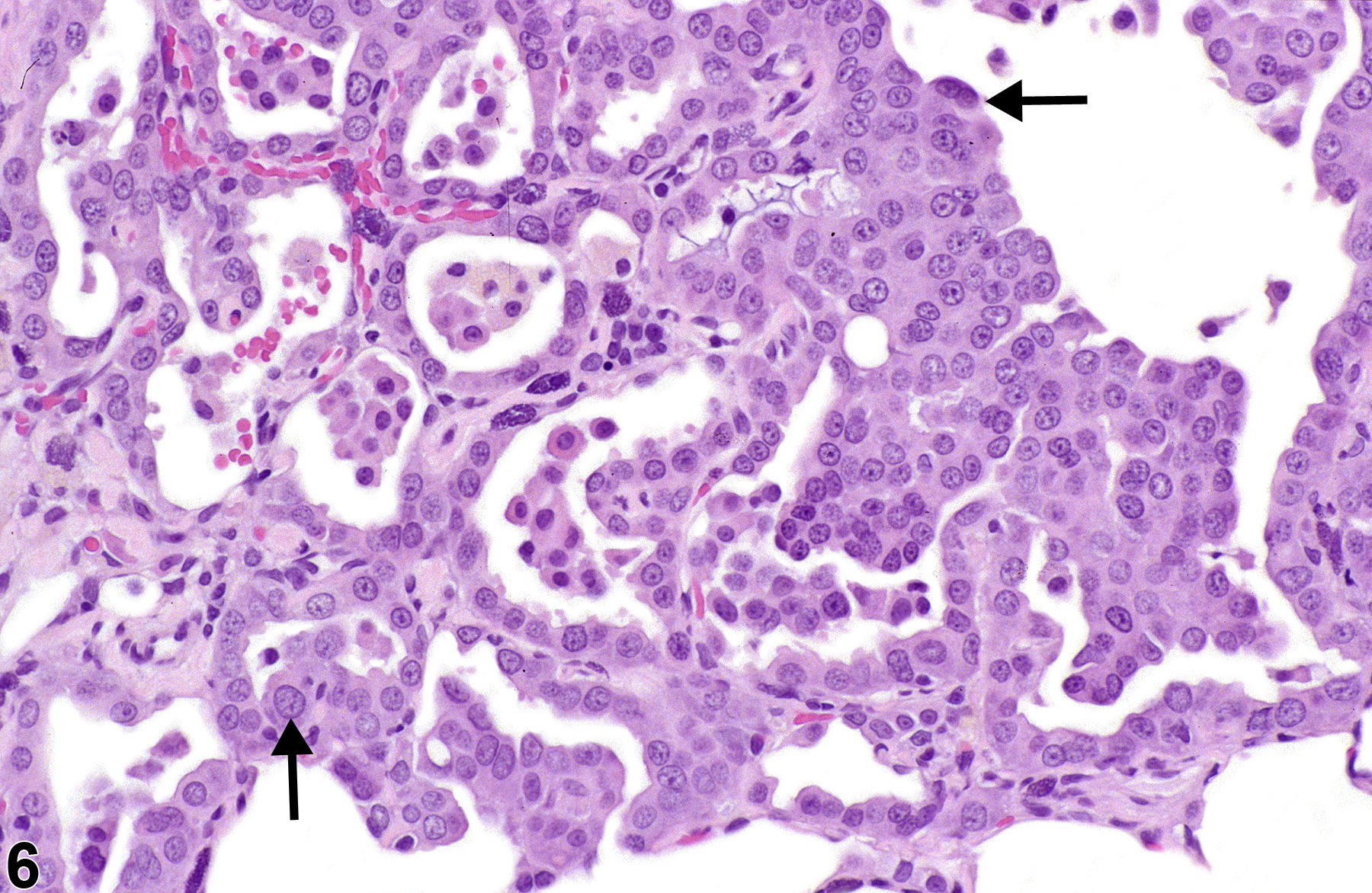
Lung, Epithelium, Alveolus - Hyperplasia, Atypical from a male F344/N rat in a chronic study. Atypical cells (arrows) are enlarged with enlarged nuclei.