

Respiratory System
Lung - Infiltration Cellular, Histiocyte
Narrative
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
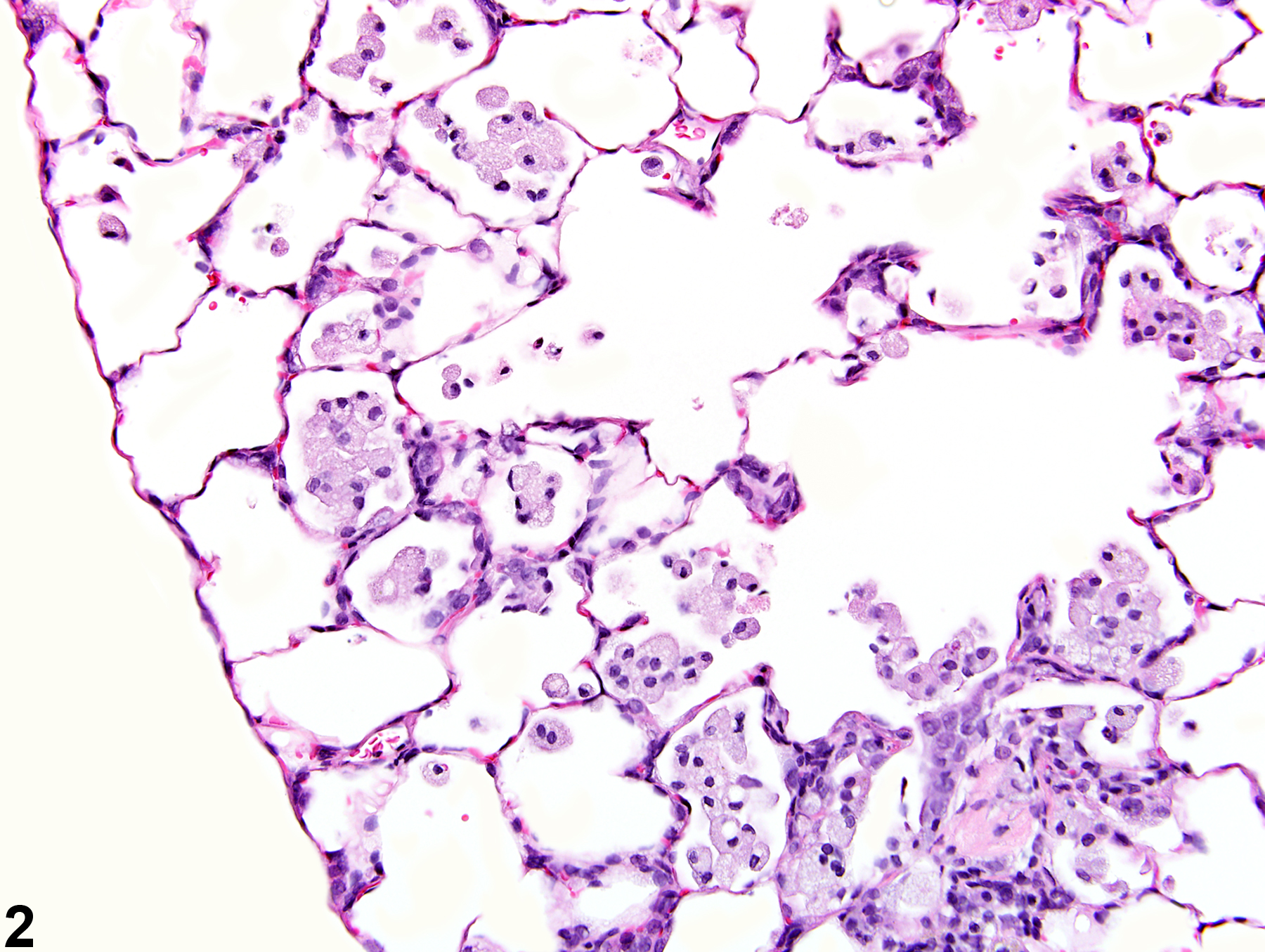
Histiocytic infiltration must be differentiated from inflammation, which can sometimes be difficult. In general, histiocytic infiltration is characterized by increased numbers of alveolar histiocytes with no (or minimal) other evidence of inflammation (e.g., the presence of other types of inflammatory cells, edema, hemorrhage, alveolar septal thickening).
Boorman GA, Eustis SL. 1990. Lung. In: Pathology of the Fischer Rat: Reference and Atlas (Boorman GA, Eustis SL, Elwell MR, Montgomery CA, MacKenzie WF, eds). Academic Press, San Diego, CA, 339-367.
Dixon D, Herbert RA, Sills RC, Boorman GA. 1999. Lungs, pleura, and mediastinum. In: Pathology of the Mouse: Reference and Atlas (Maronpot RR, Boorman GA, Gaul BW, eds). Cache River Press, Vienna, IL, 293-332.
Renne, R, Brix A, Harkema J, Herbert R, Kittle B, Lewis D, March T, Nagano K, Pino M, Rittinghausen S, Rosenbruch M, Tellier P, Wohrmann T. 2009. Proliferative and nonproliferative lesions of the rat and mouse respiratory tract. Toxicol Pathol 37(suppl):5S-73S.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/20032296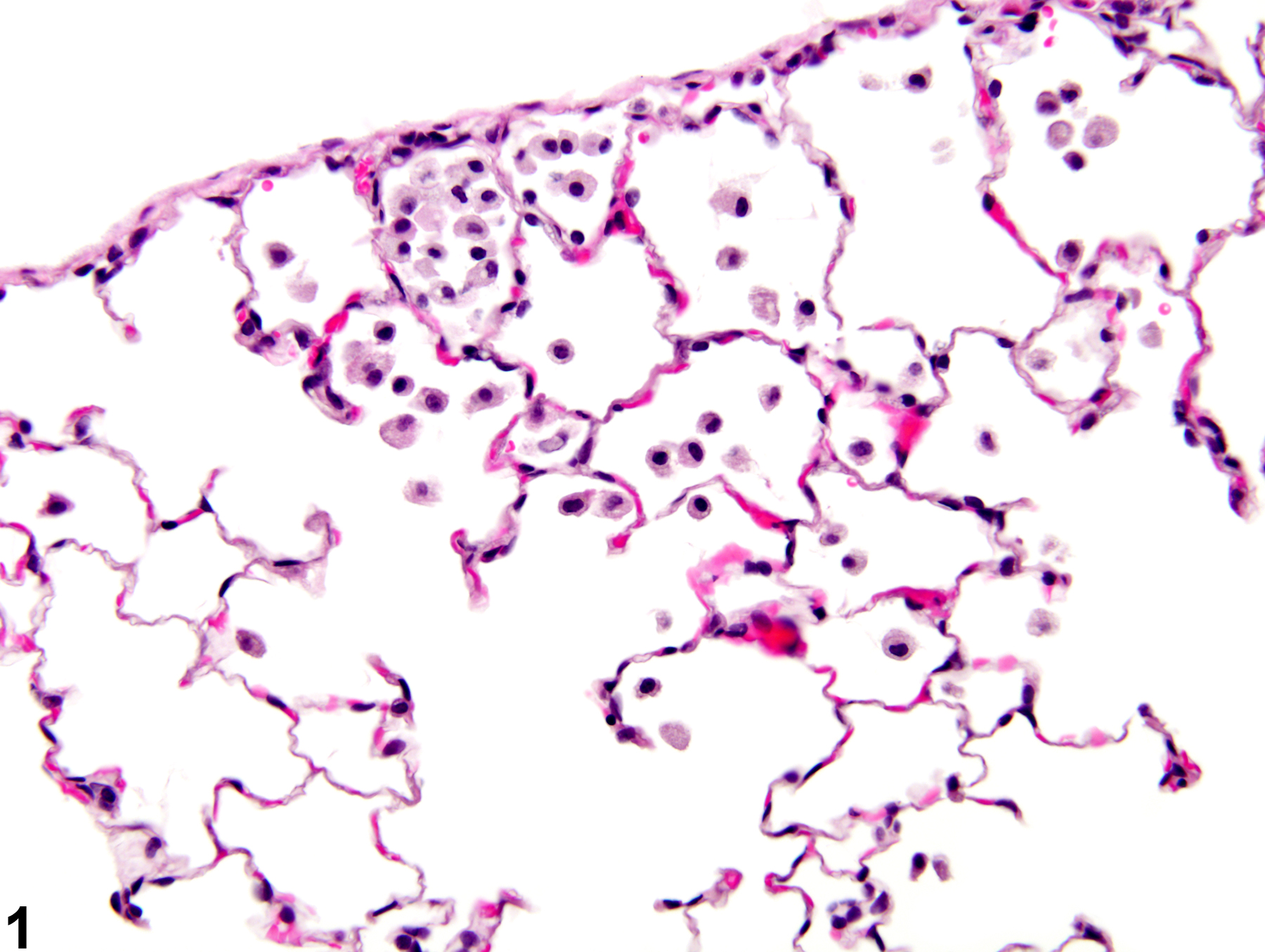
Lung - Infiltration cellular, Histiocyte in a male Wistar Han rat from a subchronic study. There is a small, subpleural accumulation of alveolar histiocytes.
All Images

Lung - Infiltration cellular, Histiocyte in a male Wistar Han rat from a subchronic study. There is a small, subpleural accumulation of alveolar histiocytes.

Lung - Infiltration cellular, Histiocyte in a female Harlan Sprague-Dawley rat from a chronic study. There is a small, subpleural accumulation of alveolar histiocytes with some thickening of associated alveolar septae.

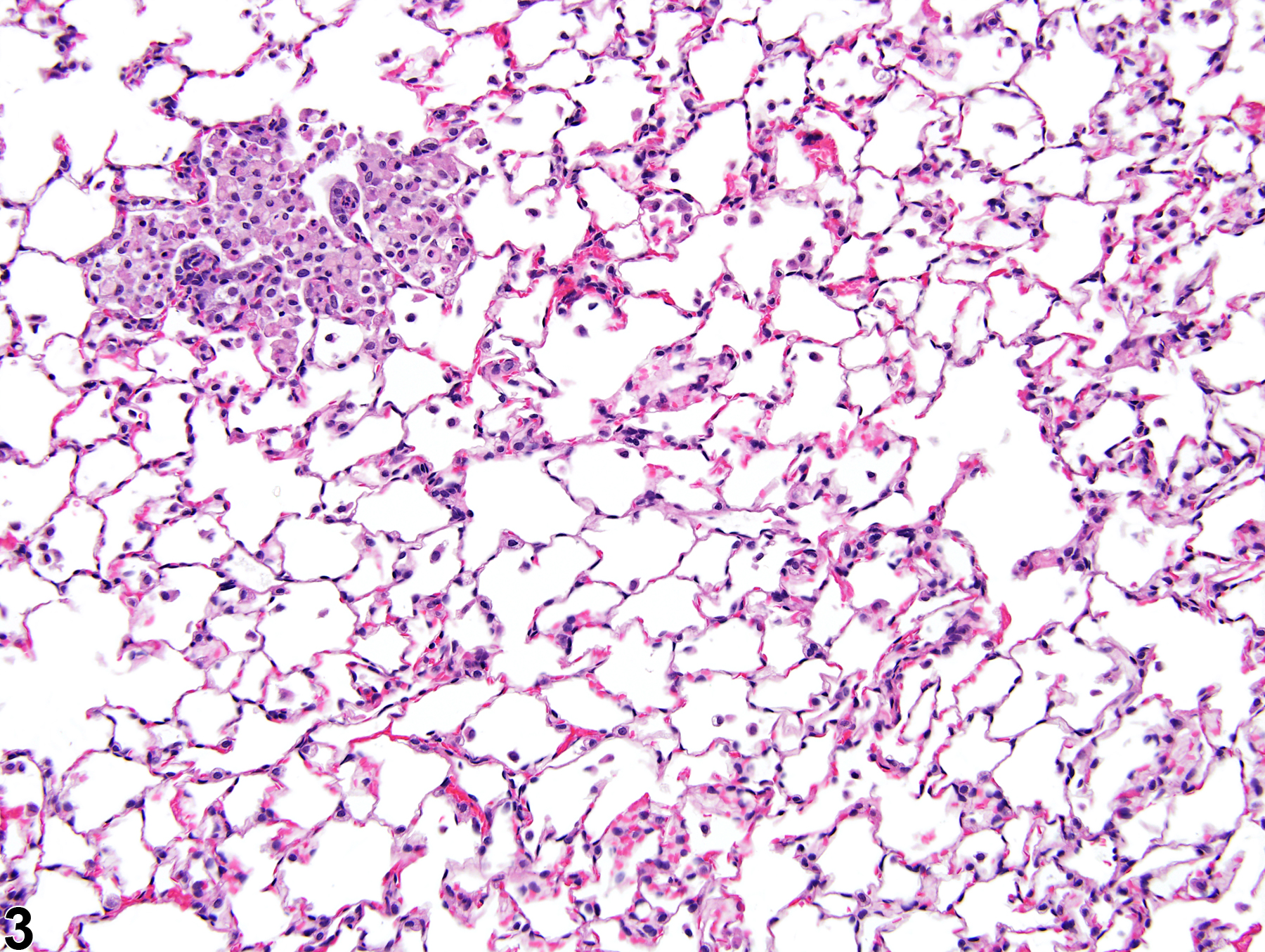
Lung - Infiltration cellular, Histiocyte in a control male F344/NTac rat from a subchronic study. There is a focal accumulation of histiocytes in several adjacent alveoli.

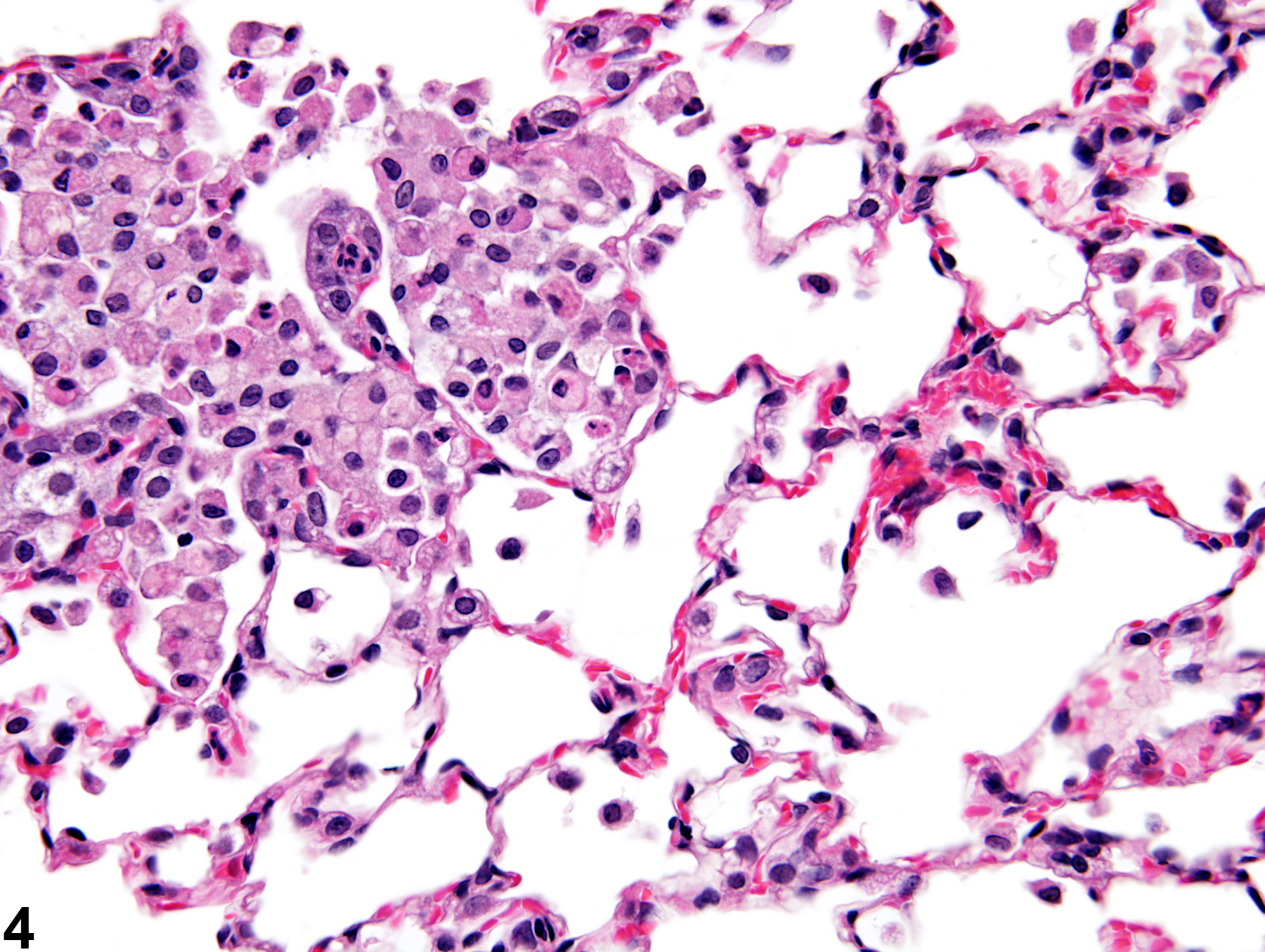
Lung - Infiltration cellular, Histiocyte in a control male F344/NTac rat form a subchronic study (higher magnification of Figure 3). Many of the alveolar macrophages in this focal accumulation contain variably sized vacuoles.

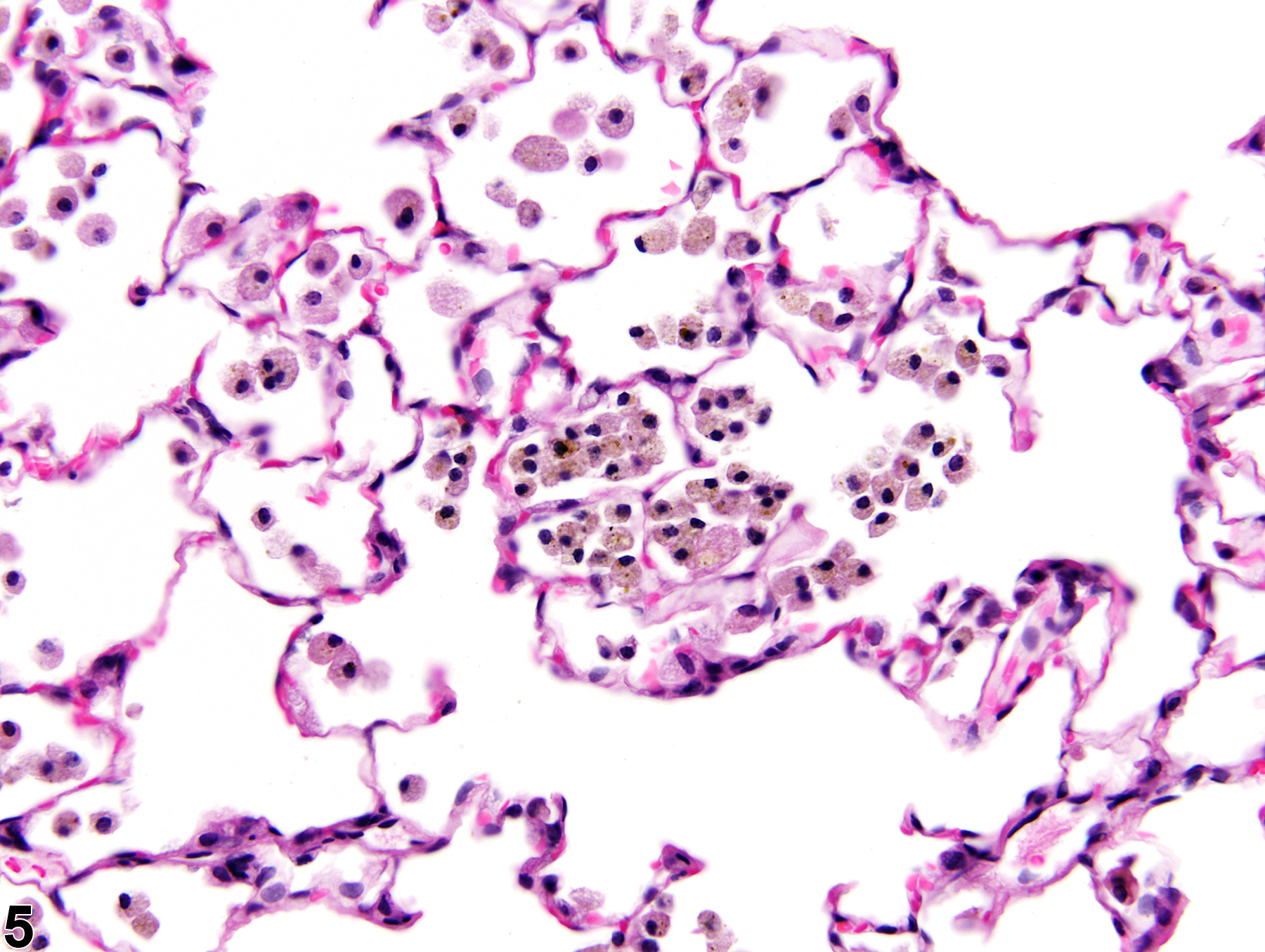
Lung - Infiltration cellular, Histiocyte in a male Wistar Han rat from a subchronic study. These histiocytes contain brown material, which is considered to be the test agent, and this animal would also be diagnosed with foreign material.

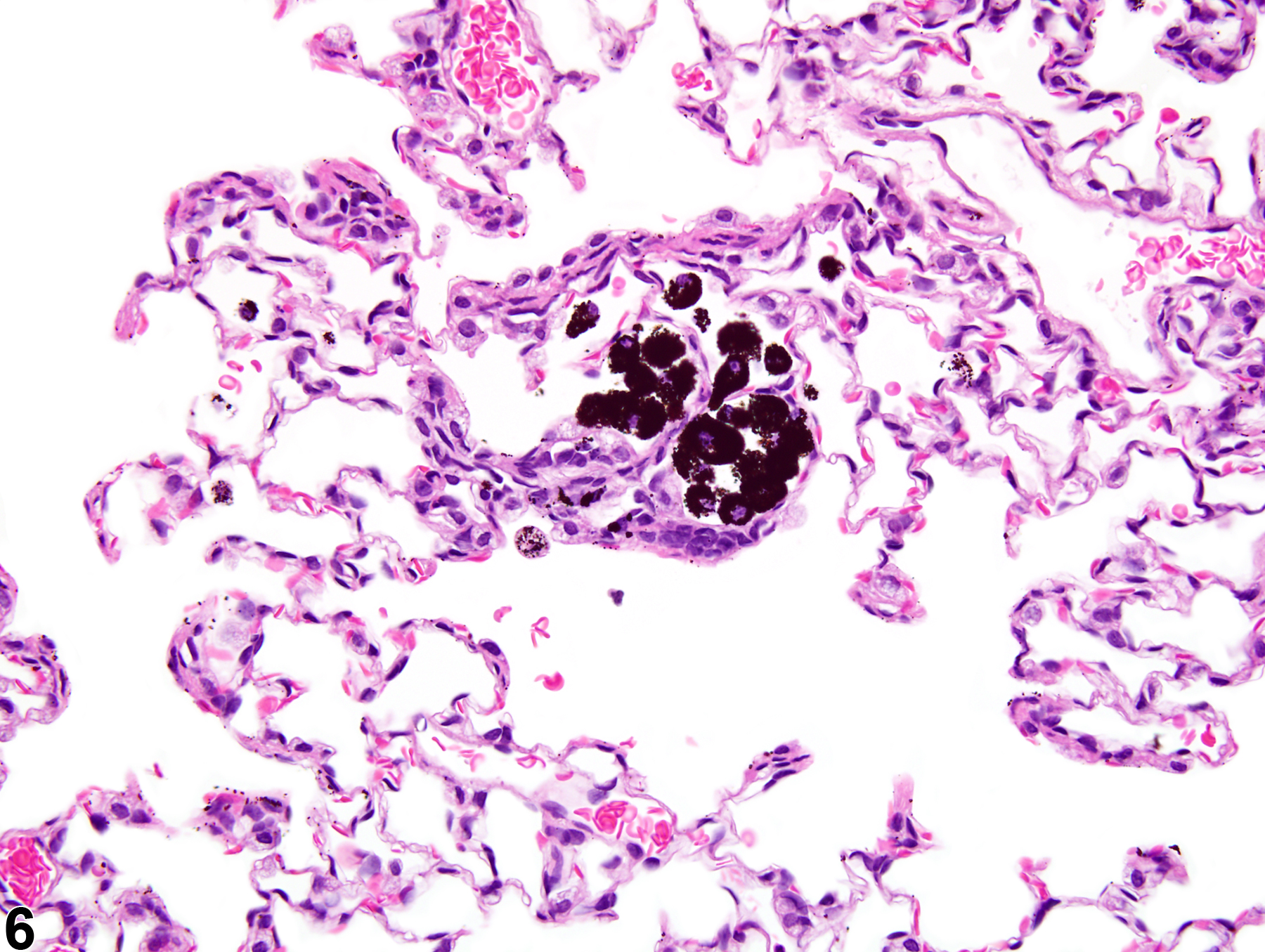
Lung - Infiltration, Cellular, Histiocyte in a male Harlan Sprague-Dawley rat from a subchronic study. These histiocytes contain black material, which is considered to be the test agent; this animal would also be diagnosed with foreign material.