

Respiratory System
Lung - Pigment
Narrative
{kind=link}
Kumar V, Abbas AK, Fausto N. 2005. Cellular adaptations, cell injury, and cell death. In: Pathologic Basis of Disease, 7th ed. Elsevier Saunders, Philadelphia, 39-40.
Pizzolato P. 1976. Formalin pigment (acid hematin) and related pigments. Am J Med Technol 42:436-440.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/790956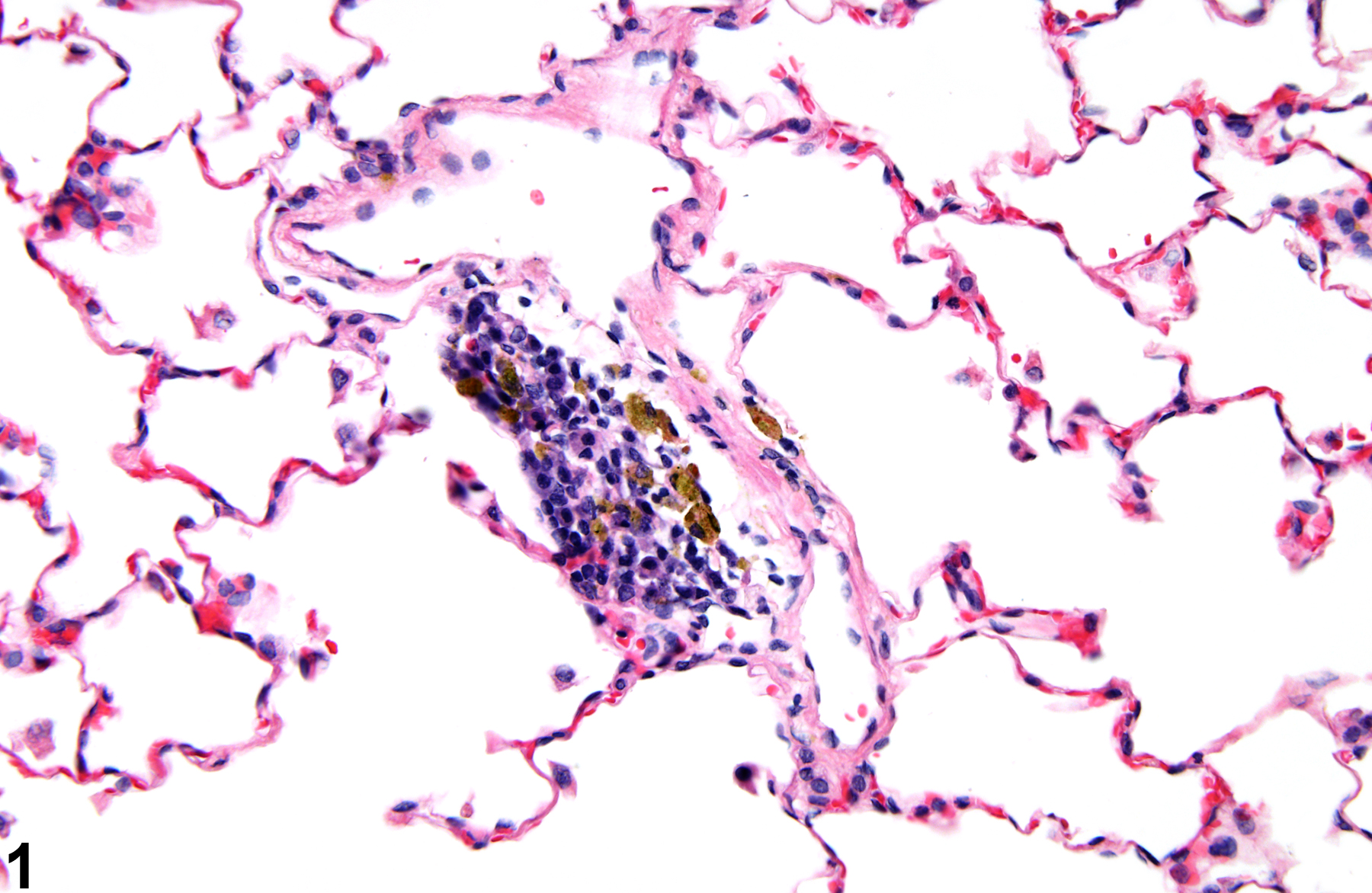
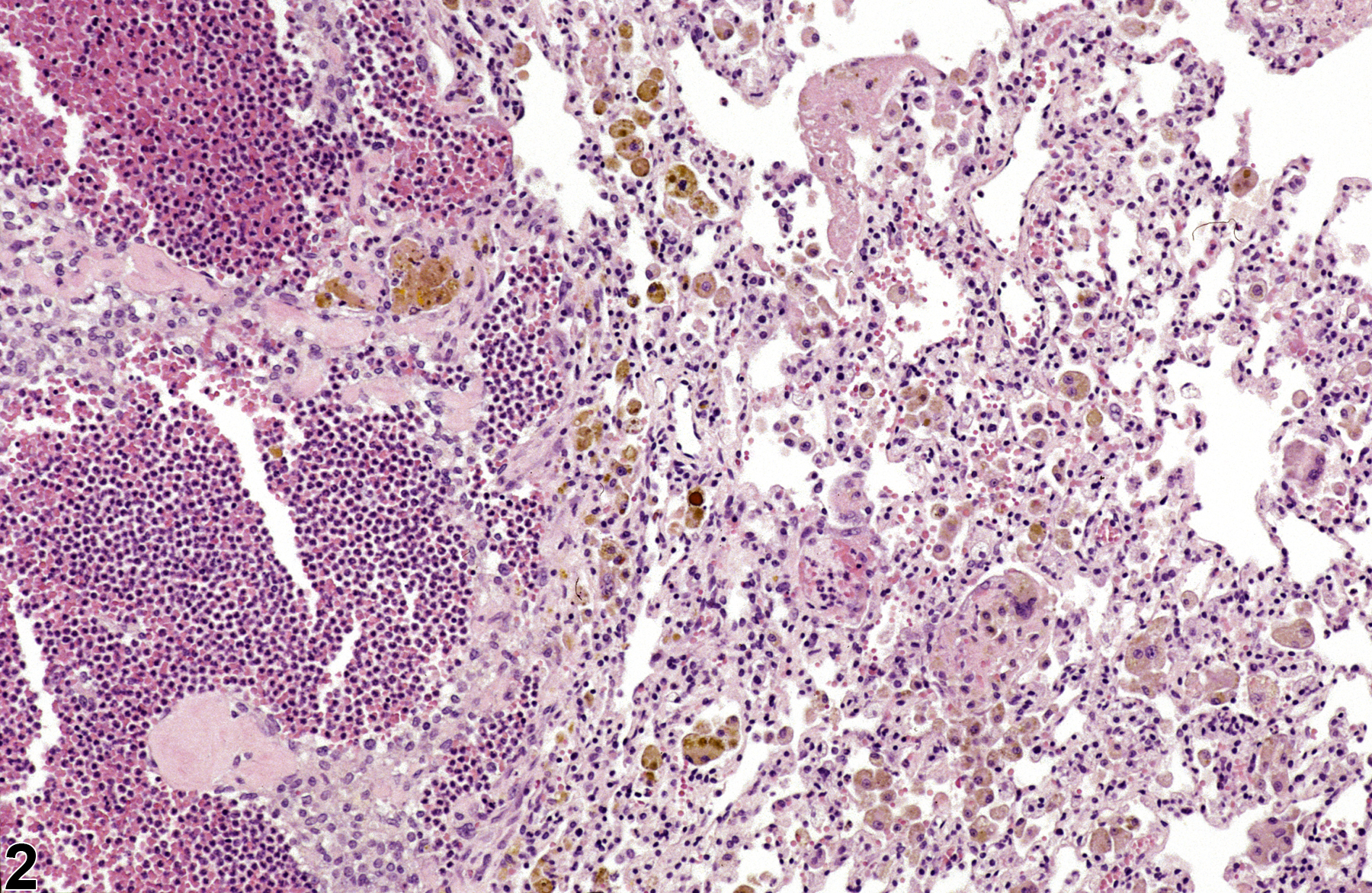
Lung, Alveolus - Pigment in a female Harlan Sprague-Dawley rat from a chronic study. The pigment is most likely hemosiderin and is contained within macrophages.
All Images

Lung, Alveolus - Pigment in a female Harlan Sprague-Dawley rat from a chronic study. The pigment is most likely hemosiderin and is contained within macrophages.

Lung - Pigment in a male F344/N rat from a chronic study. The golden brown pigment is most likely hemosiderin secondary to hemorrhage associated with acute inflammation.