

Respiratory System
Nose - Inflammation
Narrative
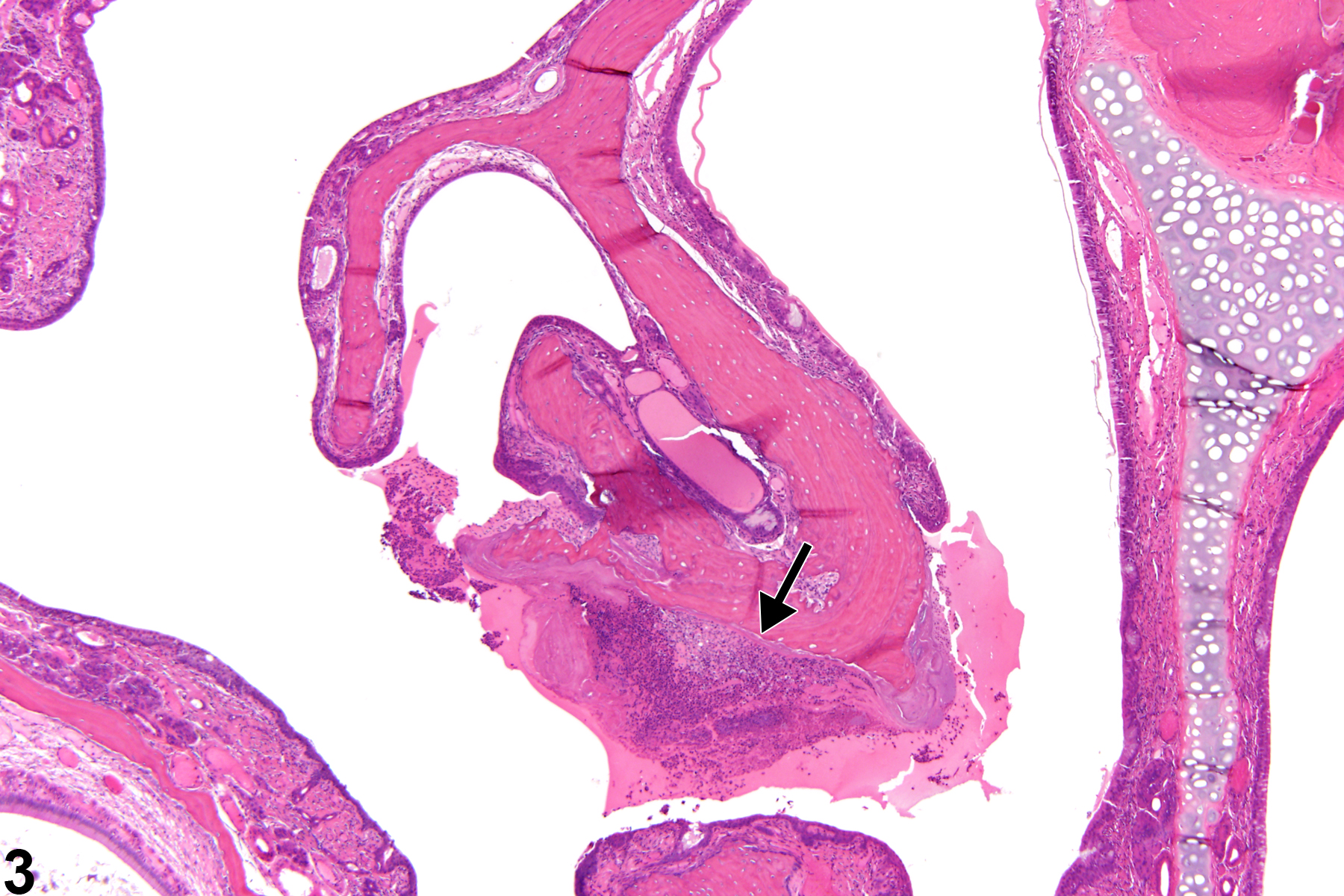
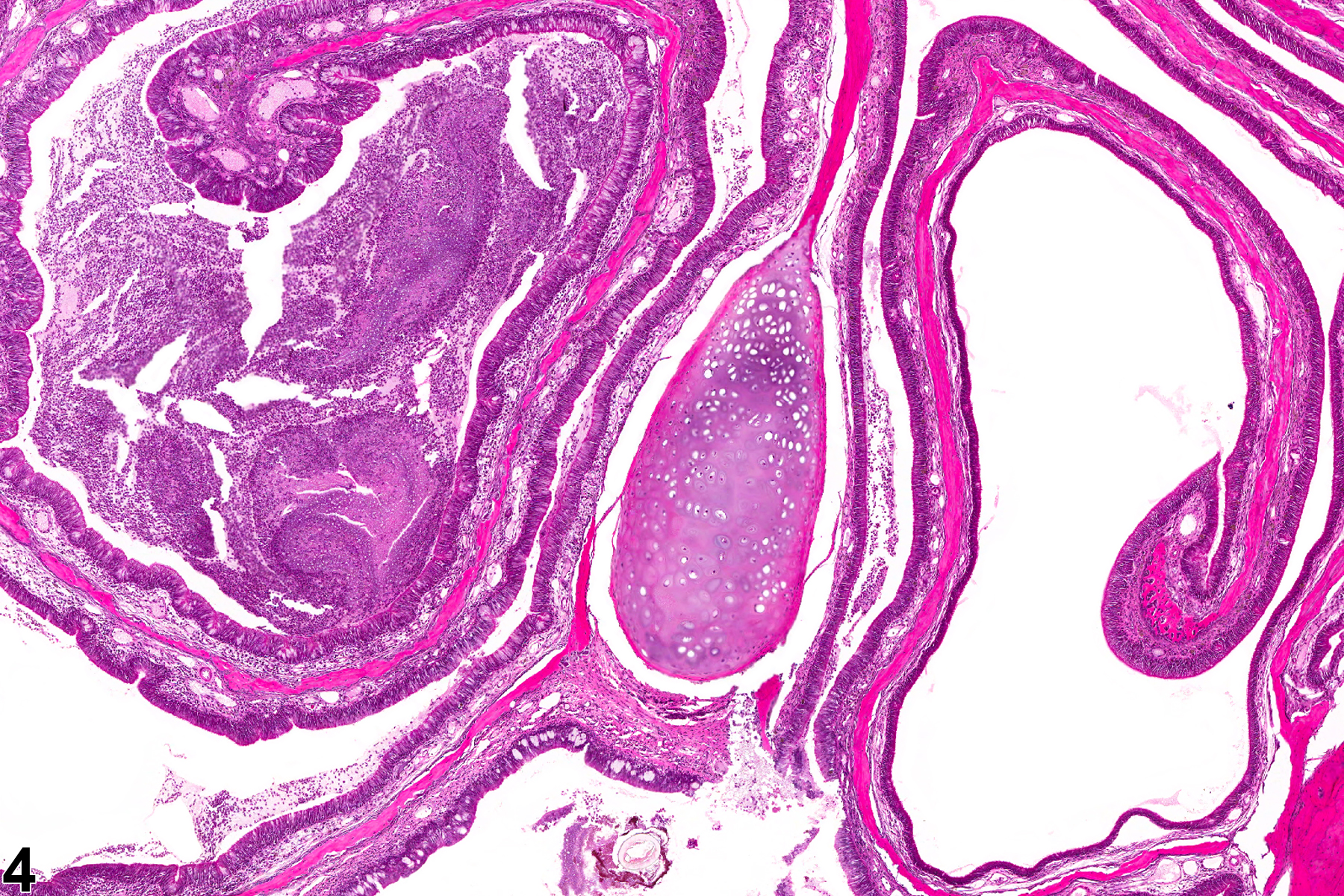
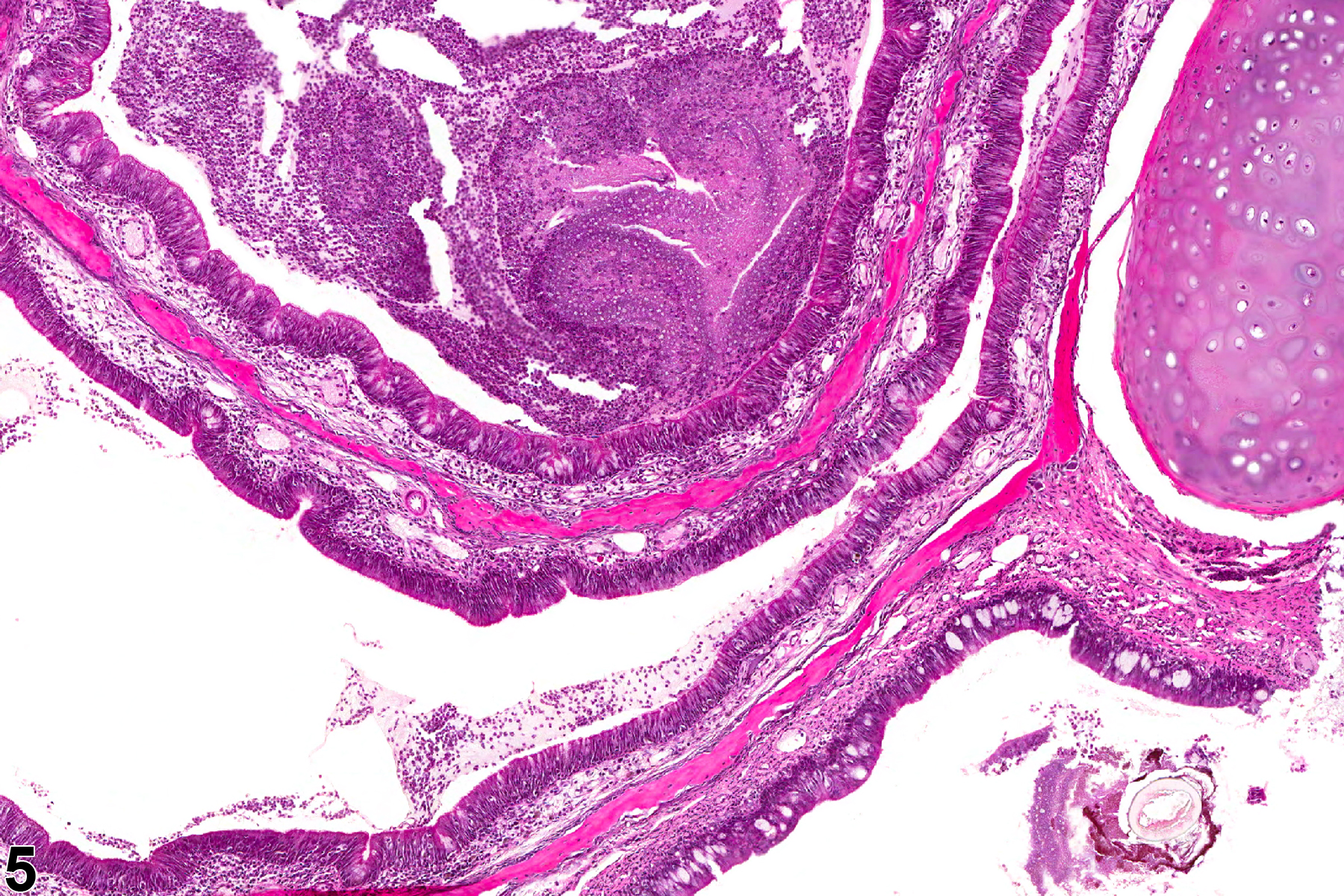
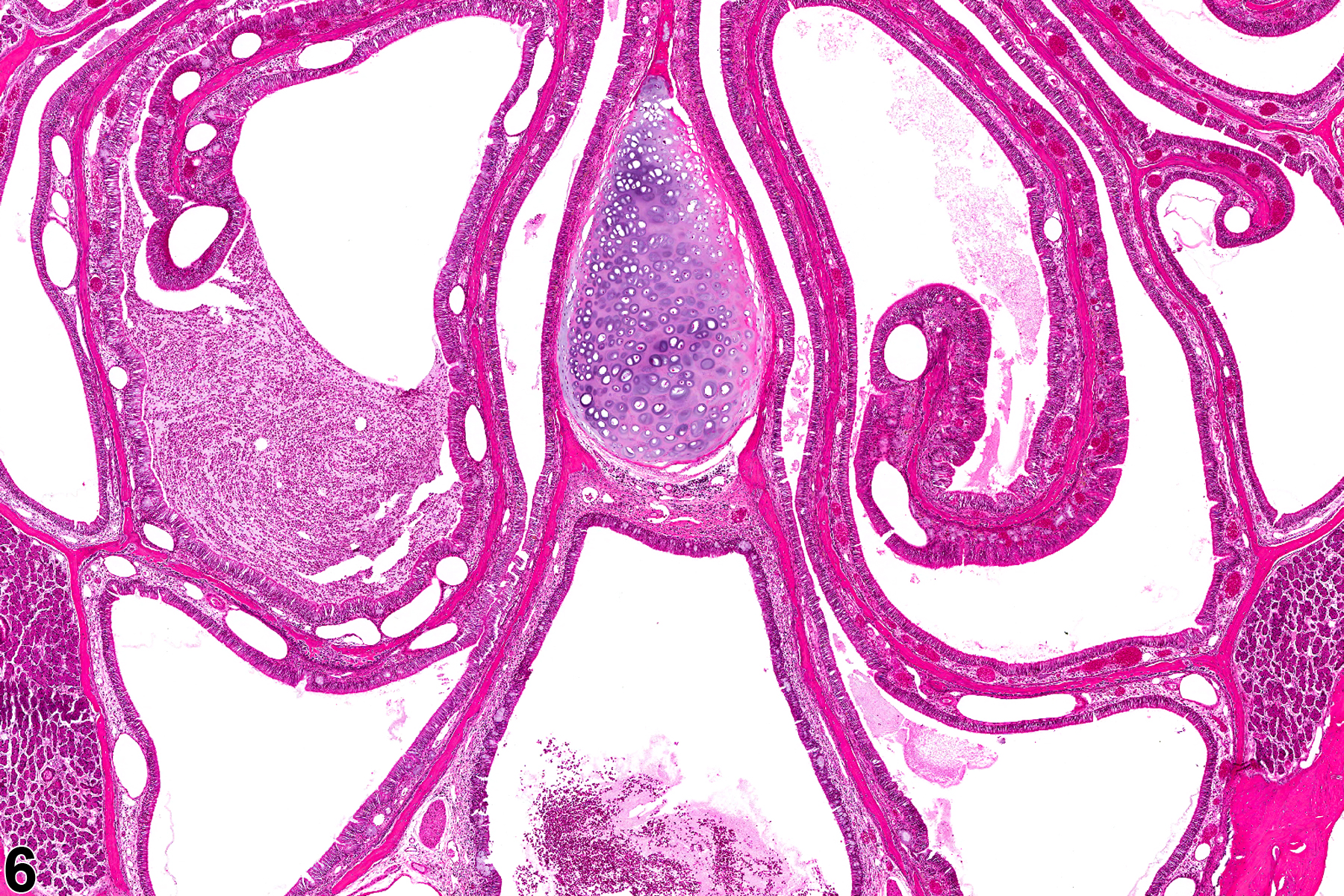
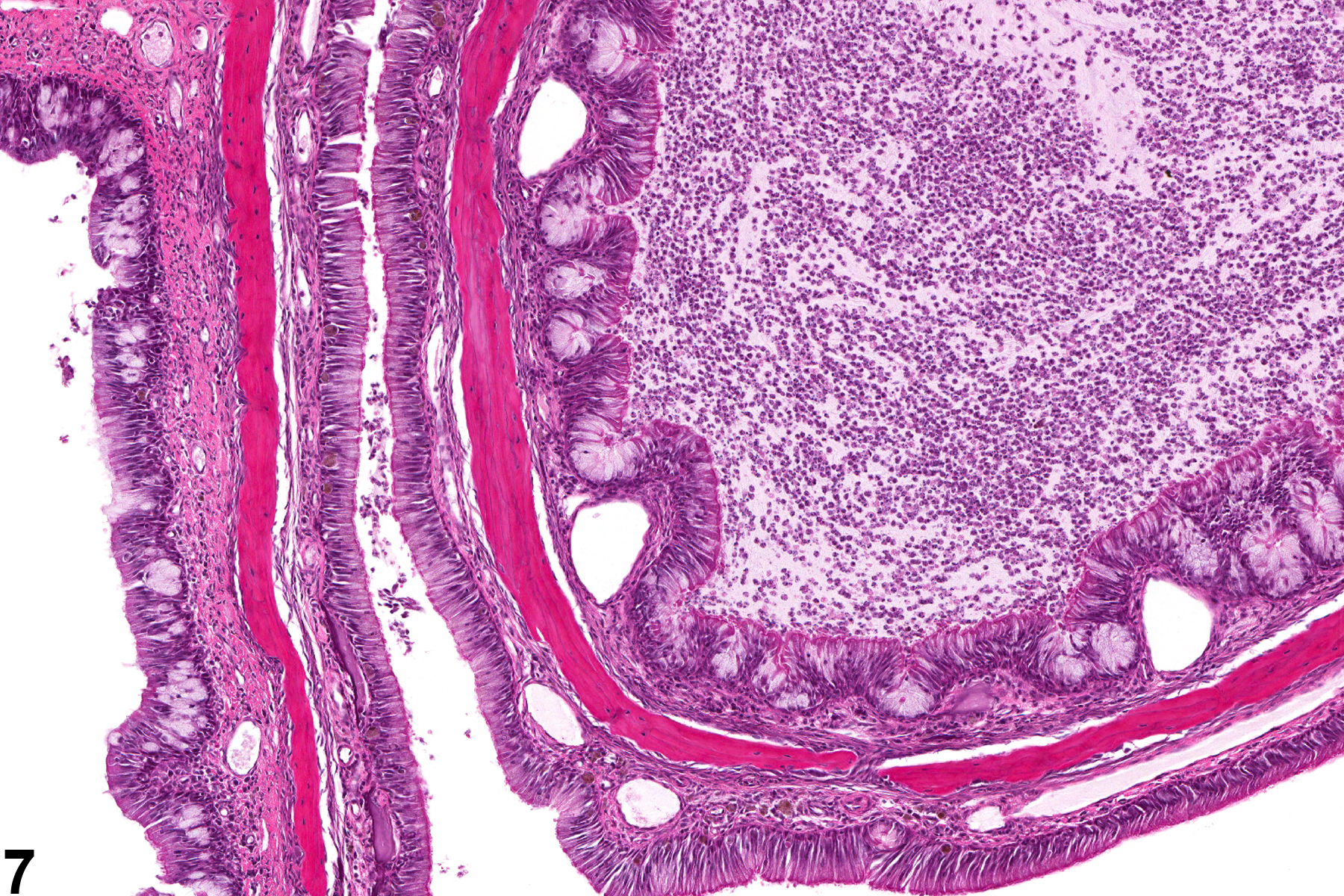
Nasal inflammation is frequently seen in conjunction with other lesions, such as necrosis, hyperplasia, metaplasia, or atrophy of the adjacent epithelium. Other associated lesions that may be causative, such as a foreign body (Figure 1) or bone necrosis in the turbinates (Figure 3) may also be seen. Reflux-induced nasal lesions need to be considered when the observed nasal lesions fit a suggestive pattern (e.g., as shown in Figure 4, Figure 5, Figure 6, and Figure 7). Reflux-related lesions tend to be more severe ventrally and laterally in the nasal cavity, less pronounced in the dorsal medial sections of the nose, and more severe in the posterior nasal sections, with severity tapered off in the anterior nasal sections. Reflux-induced nasal lesions may have a unilateral predominance.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Boorman GA, Morgan KT, Uraih LC. 1990. Nose, larynx, and trachea. In: Pathology of the Fischer Rat: Reference and Atlas (Boorman GA, Eustis SL, Elwell MR, eds). Academic Press, San Diego, 315-337.
Damsch S, Eichenbaum G, Looszova A, Lammens L, Feyen B, Van den Bulck K, Knight E, Kelley M, Tonelli A. 2011. Unexpected nasal changes in rats related to reflux after gavage dosing. Toxicol Pathol 39:337-347.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/21422260Damsch S, Eichenbaum G, Tonelli A, Lammens L, Van den Bulck K, Feyen B, Vandenberghe J, Megens A, Knight E, Kelley M. 2011. Gavage-related reflux in rats: Identification, pathogenesis, and toxicological implications. Toxicol Pathol 39:348-360.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/21422261Eichenbaum G, Damsch S, Looszova A, Vandenberghe J, Van den Bulck K, Roels K, Megens A, Knight E, Hillsamer V, Feyen B, Kelley MF, Tonelli A, Lammens L. 2011. Impact of gavage dosing procedure and gastric content on adverse respiratory effects and mortality in rat toxicity studies. J Appl Toxicol 31:342-354.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/21089156Herbert RA, Leninger JR. 1999. Nose, larynx, and trachea. In: Pathology of the Mouse: Reference and Atlas (Maronpot RR, ed). Cache River Press, Vienna, IL, 259-292.
National Toxicology Program. 2011. NTP TR-564. Toxicology and Carcinogenesis Studies of 1-Bromopropane (CAS No. 106-94-5) in F344/N Rats and B6C3F1 Mice (Inhalation Studies). NTP, Research Triangle Park, NC.
Abstract: https://ntp.niehs.nih.gov/go/34854National Toxicology Program. 2011. NTP TR-566. Toxicology and Carcinogenesis Studies of Diethylamine (CAS No. 109-89-7) in F344/N Rats and B6C3F1 Mice (Inhalation Studies). NTP, Research Triangle Park, NC.
Abstract: https://ntp.niehs.nih.gov/go/34820Renne R, Brix A, Harkema J, Kittel B, Lewis D, March T, Nagano K, Pino M, Rittinghausen S, Rosenbruch M, Tellier P, Wohrmann T. 2009. Proliferative and nonproliferative lesions of the rat and mouse respiratory tract. Toxicol Pathol 37(7 suppl):5S-73S.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/20032296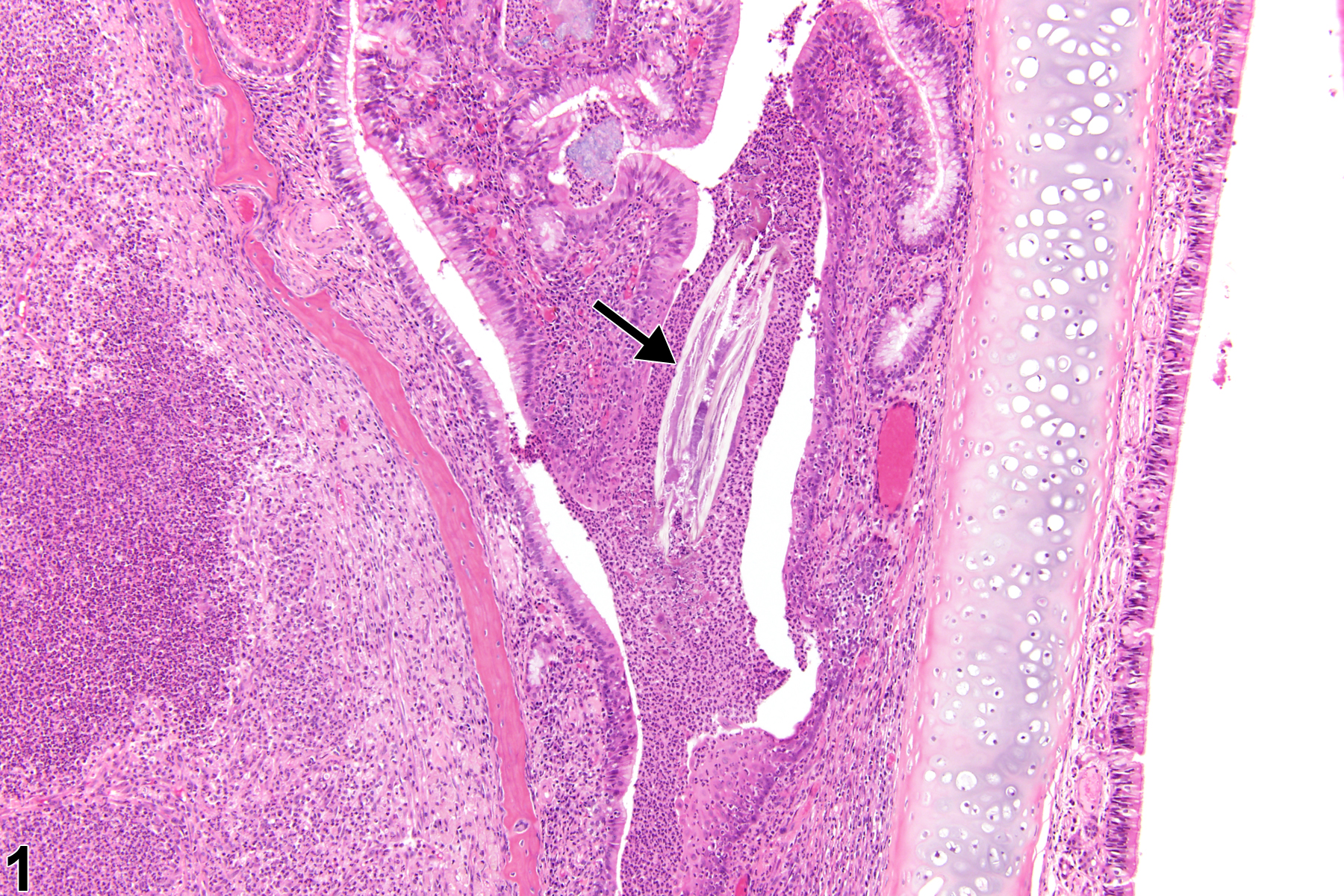
Nose, Respiratory epithelium - Inflammation, Suppurative in a male F344/N rat from a chronic study. This lesion is a unilateral, ventral, suppurative inflammatory cell response that contains a foreign body (arrow).
All Images

Nose, Respiratory epithelium - Inflammation, Suppurative in a male F344/N rat from a chronic study. This lesion is a unilateral, ventral, suppurative inflammatory cell response that contains a foreign body (arrow).
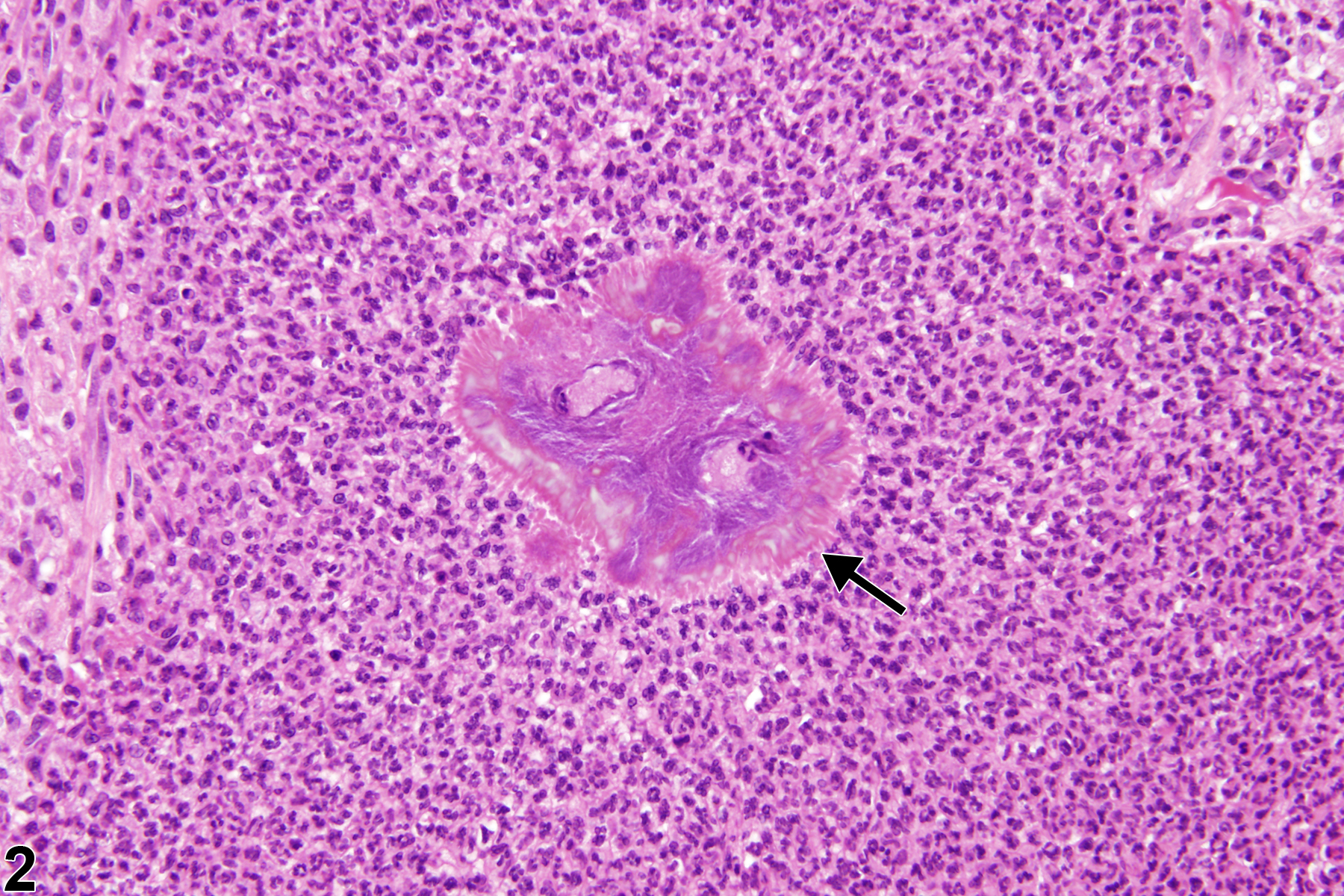
Nose, Respiratory epithelium - Inflammation, Suppurative in a male F344/N rat from a chronic study (higher magnification of Figure 1). Splendore-Hoeppli material (arrow) is present in the neutrophilic infiltrate.

Nose, Respiratory epithelium - Inflammation, Suppurative in a male F344/N rat from a chronic study. The suppurative inflammation in the ventral nasal cavity is associated with bone necrosis (arrow).

Nose, Olfactory epithelium - Inflammation, Suppurative in a female F344/N rat from a chronic study. There is a proliferative epithelial reaction to the suppurative inflammation in the ventral nasal cavity.

Nose, Olfactory epithelium - Inflammation, Suppurative in a female F344/N rat from a chronic study (higher magnification of Figure 4). Epithelial hyperplasia is associated with the suppurative inflammation in the ventral nasal cavity.

Nose, Olfactory epithelium - Inflammation, Suppurative, and Nose, Respiratory epithelium - Inflammation, Suppurative in a male F344/N rat from a chronic study. In addition to the suppurative reaction in the nasal cavity, the nasopharyngeal duct is also affected.

Nose, Olfactory epithelium - Inflammation, Suppurative in a male F344/N rat from a chronic study. A pronounced epithelial proliferative reaction is present secondary to the suppurative inflammation.
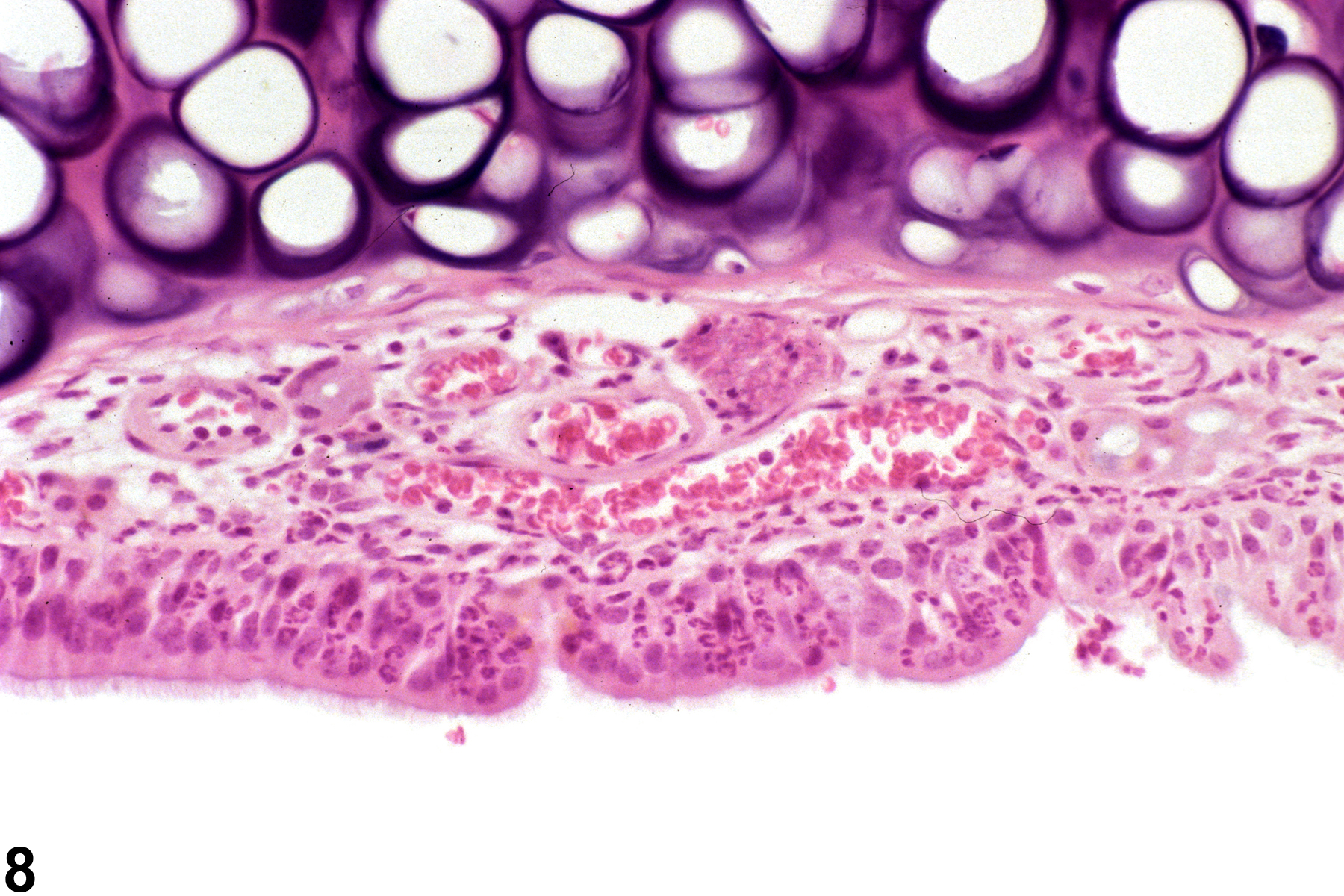
Nose, Respiratory epithelium - Inflammation, Acute in a male B6C3F1/N mouse from a chronic study. Neutrophils are present within the mucosal epithelium.
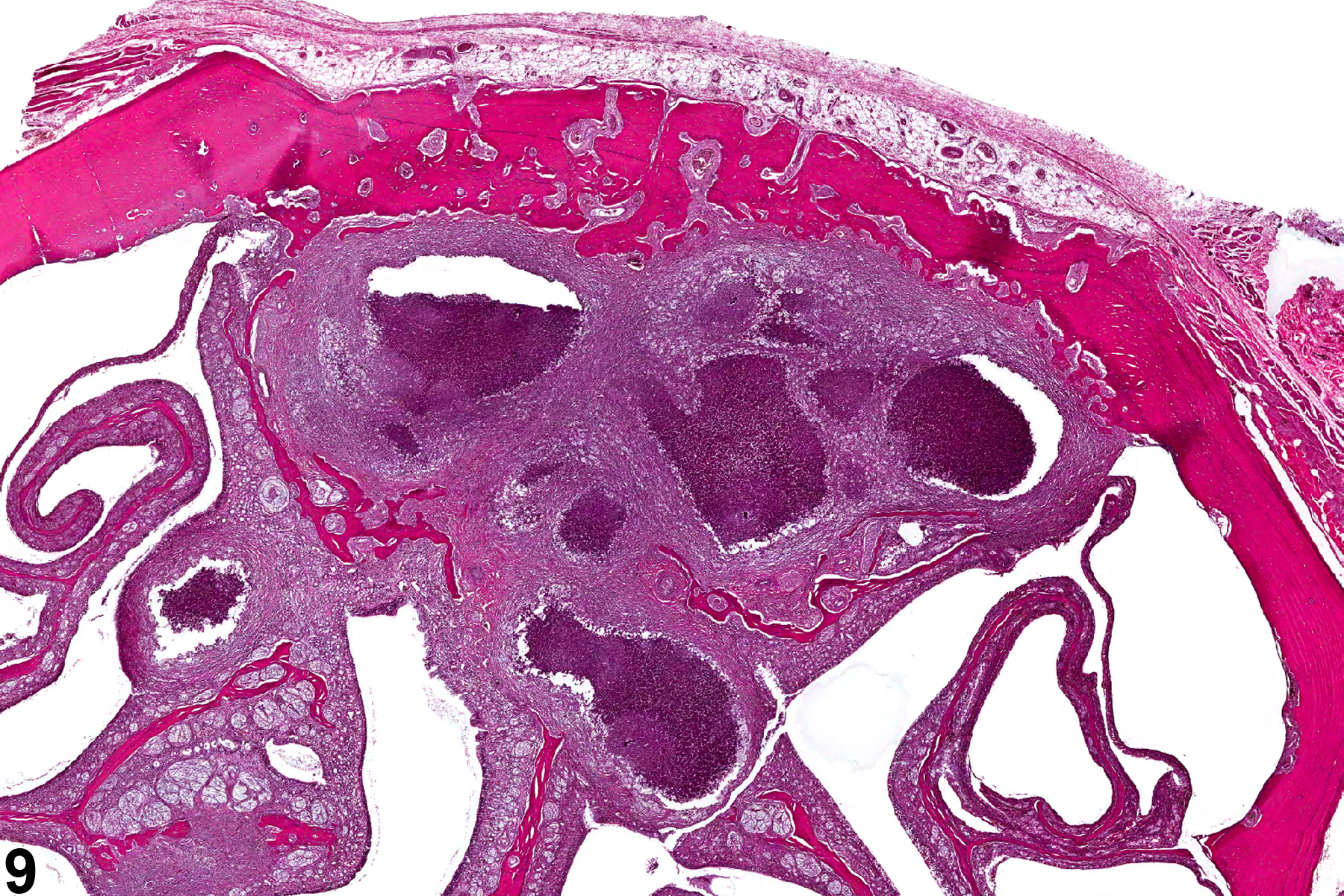
Nose, Olfactory epithelium - Inflammation, Suppurative in a male F344/N rat from a chronic study. This nest of abscesses is a category of suppurative inflammation in which the neutrophilic infiltrates are walled off by connective tissue.
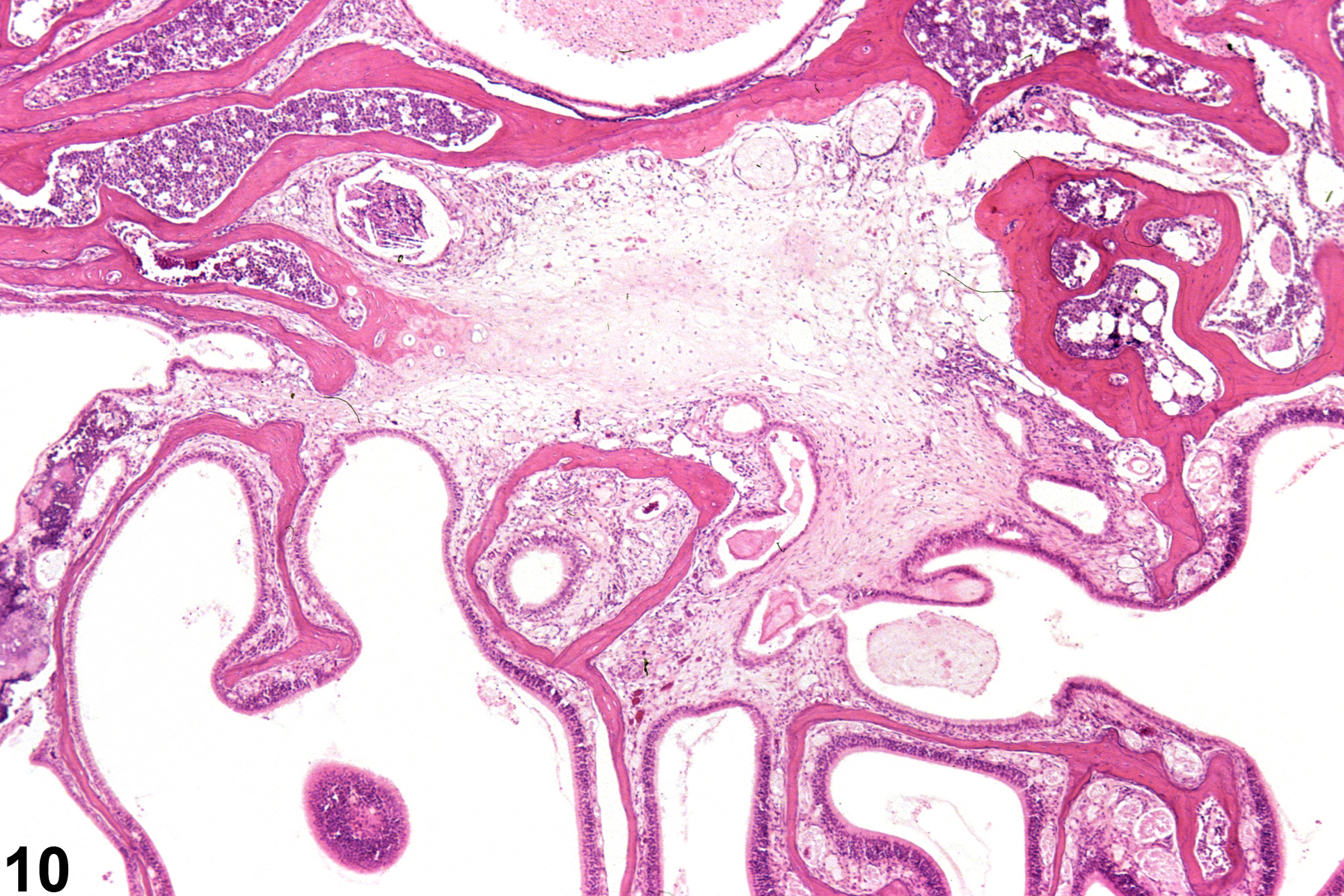
Nose, Olfactory epithelium - Inflammation, Chronic in a male B6C3F1/N mouse from a chronic study. Chronic inflammation characterized by exuberant fibrosis is present in the posterior nasal cavity.
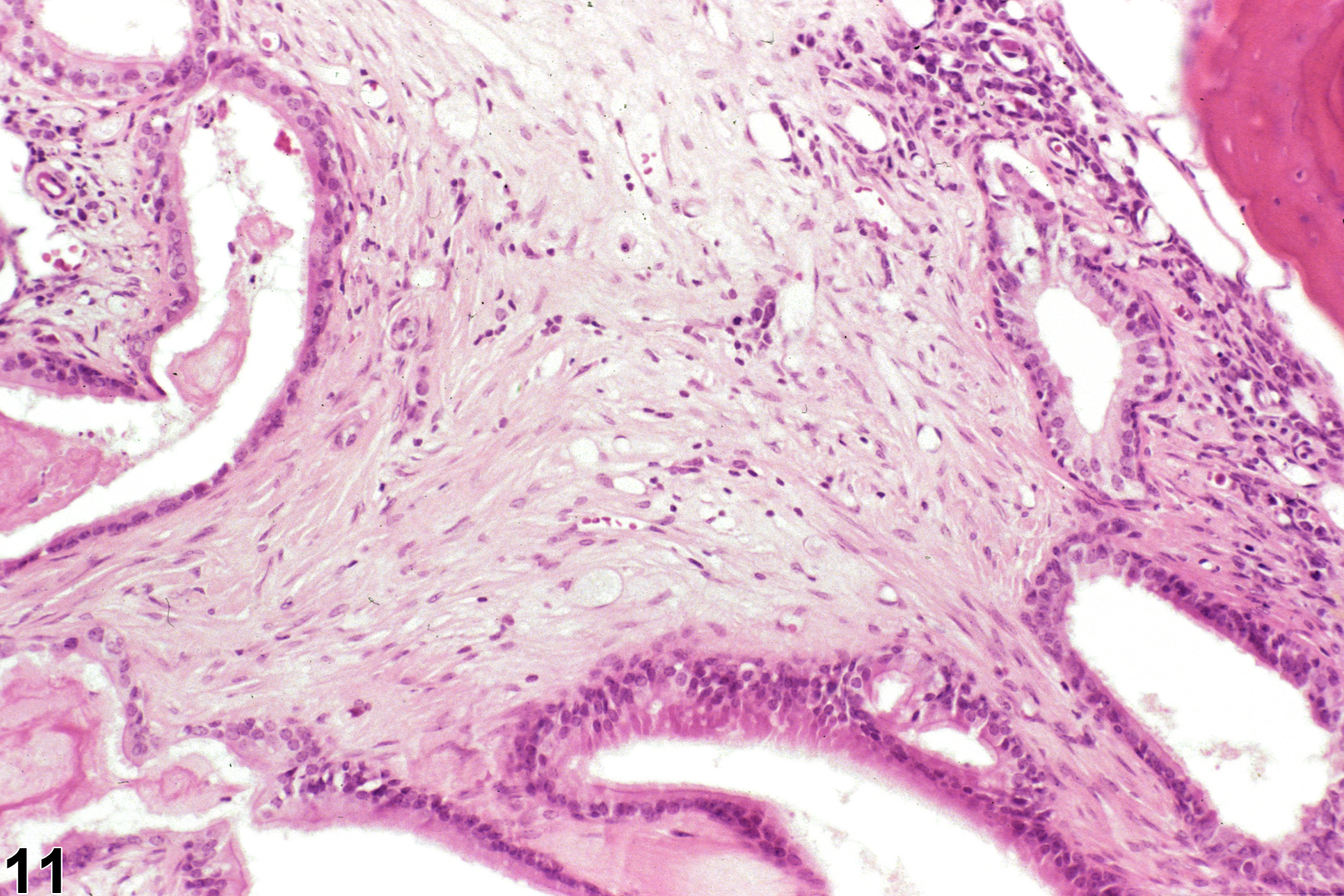
Nose, Olfactory epithelium - Inflammation, Chronic in a male B6C3F1/N mouse from a chronic study (higher magnification of Figure 10). Some inflammatory cells are associated with the fibrosis in the posterior nasal cavity.