

Urinary System
Kidney - Fibrosis
Narrative
{kind=link}
Cavallo T. 1998. Tubulointerstitial nephritis. In: Heptinstall’s Pathology of the Kidney, 5th ed (Jennette JC, Olson JL, Schwartz MM, Silva FG, eds). Lippincott-Raven, Philadelphia, 667-723.
Eddy AA. 1996. Molecular insights into renal interstitial fibrosis. J Am Soc Nephrol 7:2495-2508.
Abstract: http://www.ncbi.nlm.nih.gov/pubmed/8989727Frazier KS, Dube P, Paredes A, Styer E. 2000. Connective tissue growth factor expression in the rat remnant kidney model and association with tubular epithelial cells undergoing transdifferentiation. Vet Pathol 37:328-335.
Full Text: http://vet.sagepub.com/content/37/4/328.full.pdfYamate J, Sato K, Machida Y, Ide M, Sato S, Nakatsuji S, Kuwamura M, Kotani T, Sakuma S. 2000. Cisplatin-induced rat renal interstitial fibrosis: A possible pathogenesis based on the data. J Toxicol Pathol 13:237-247.
Full Text: http://tpx.sagepub.com/content/33/2/207.longYang J, Liu Y. 2001. Dissection of key events in tubular epithelial to myofibroblast transition and its implications in renal interstitial fibrosis. Am J Pathol 159:1465-1475.
Full Text: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1850509/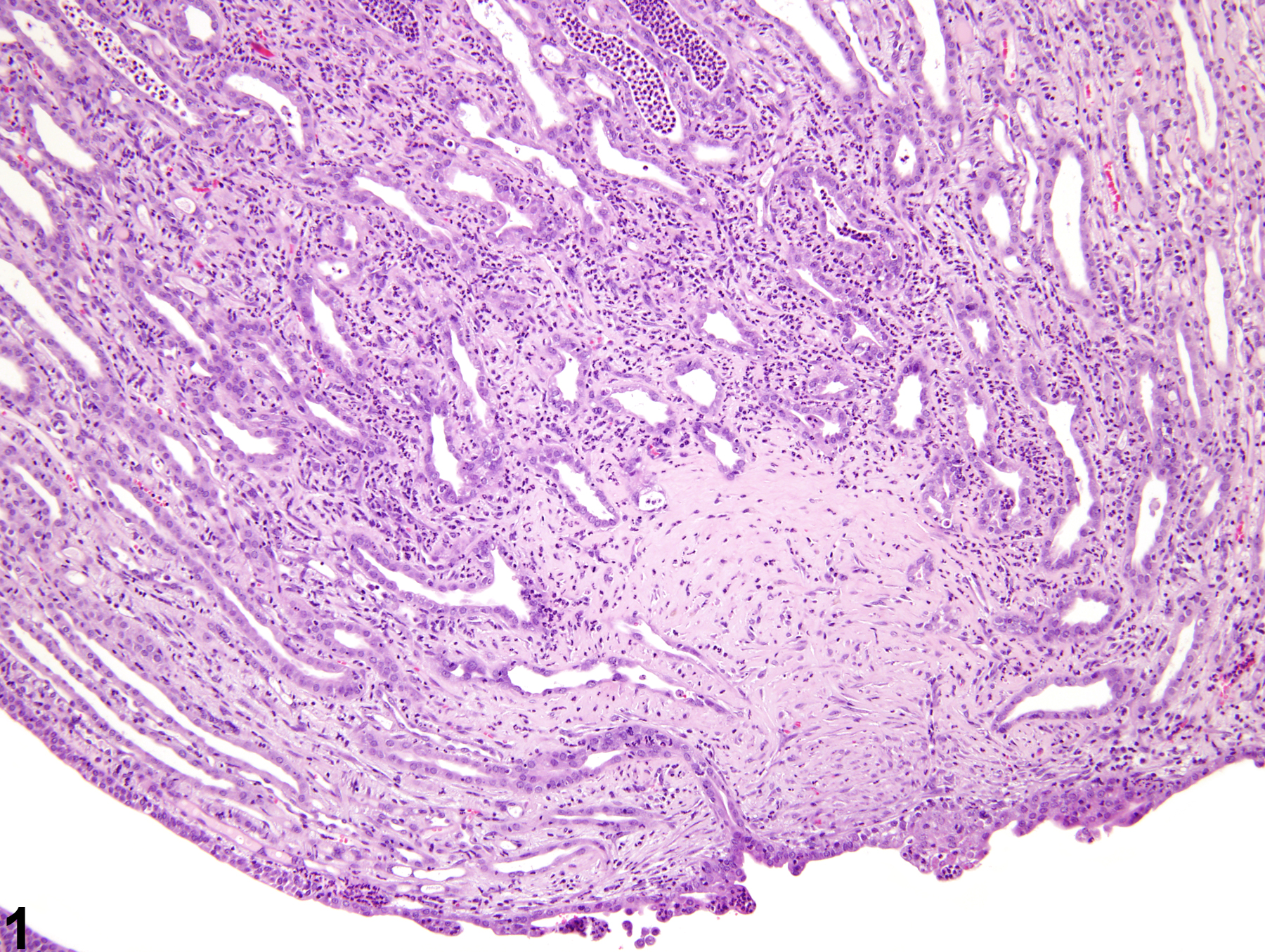
Kidney - Fibrosis in a female F344/N rat from a chronic study. A focal area of fibrosis is present in the distal renal papilla.
All Images

Kidney - Fibrosis in a female F344/N rat from a chronic study. A focal area of fibrosis is present in the distal renal papilla.

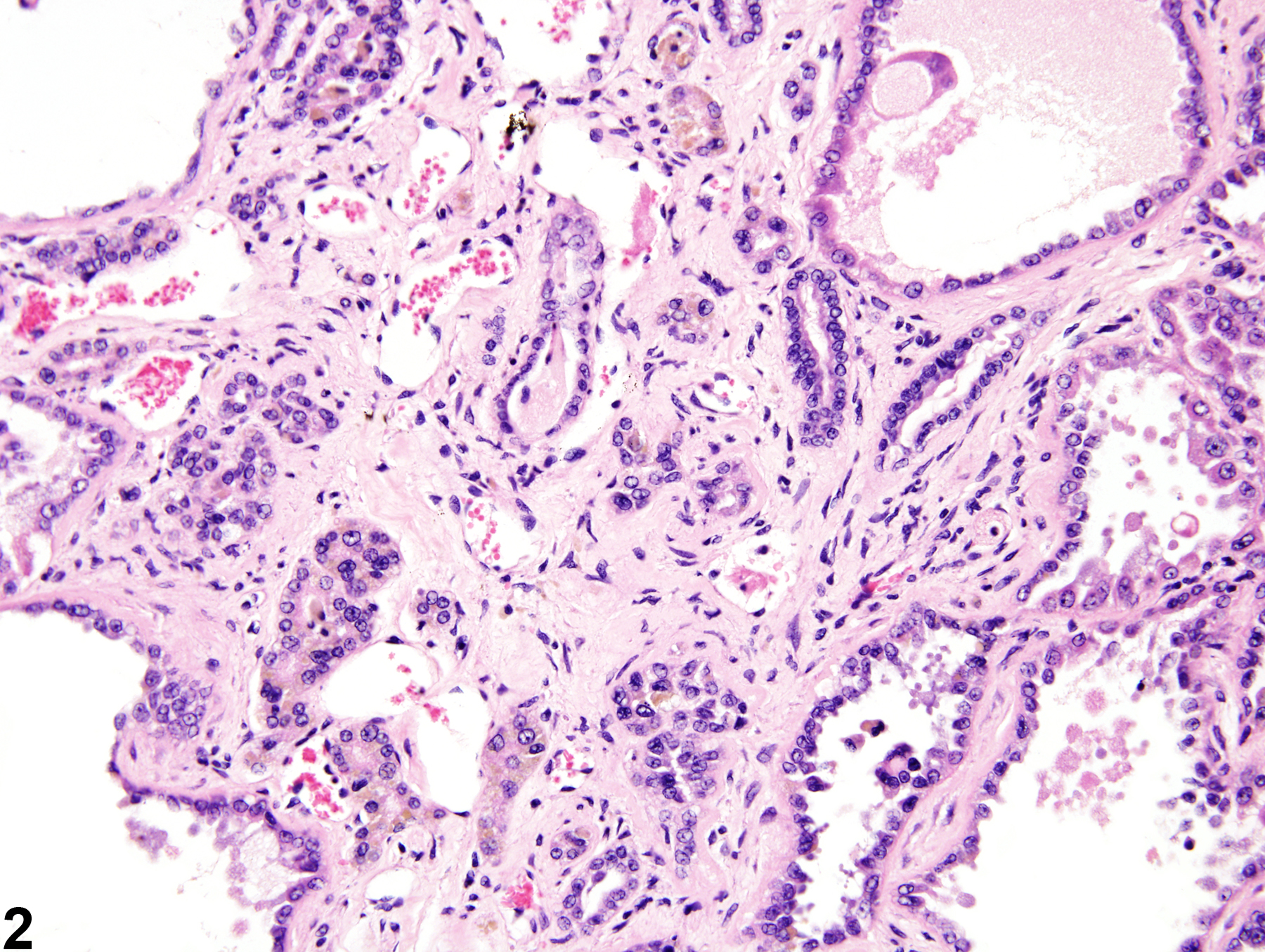
Kidney - Fibrosis in a male F344/N rat from a chronic study. Interstitial fibrosis separates renal tubules.