

Urinary System
Kidney - Infarct
Narrative
{kind=link}
{kind=link}
Hard GC, Alden CL, Bruner RH, Frith CH, Lewis RM, Owen RA, Krieg K, Durchfeld-Meyer B. 1999. Non-proliferative lesions of the kidney and lower urinary tract in rats. In: Guides for Toxicologic Pathology. STP/ARP/AFIP, Washington, DC, 1-32.
Montgomery CA, Seely JC. 1990. Kidney. In: Pathology of the Fischer Rat: Reference and Atlas (Boorman GA, Eustis SL, Elwell MR, Montgomery CA, MacKenzie WF, eds). Academic Press, San Diego, 127-153.
Abstract: http://www.ncbi.nlm.nih.gov/nlmcatalog/9002563Seely JC. 1999. Kidney. In: Pathology of the Mouse: Reference and Atlas (Maronpot RR, Boorman GA, Gaul BW, eds). Cache River Press, Vienna, IL, 207-234.
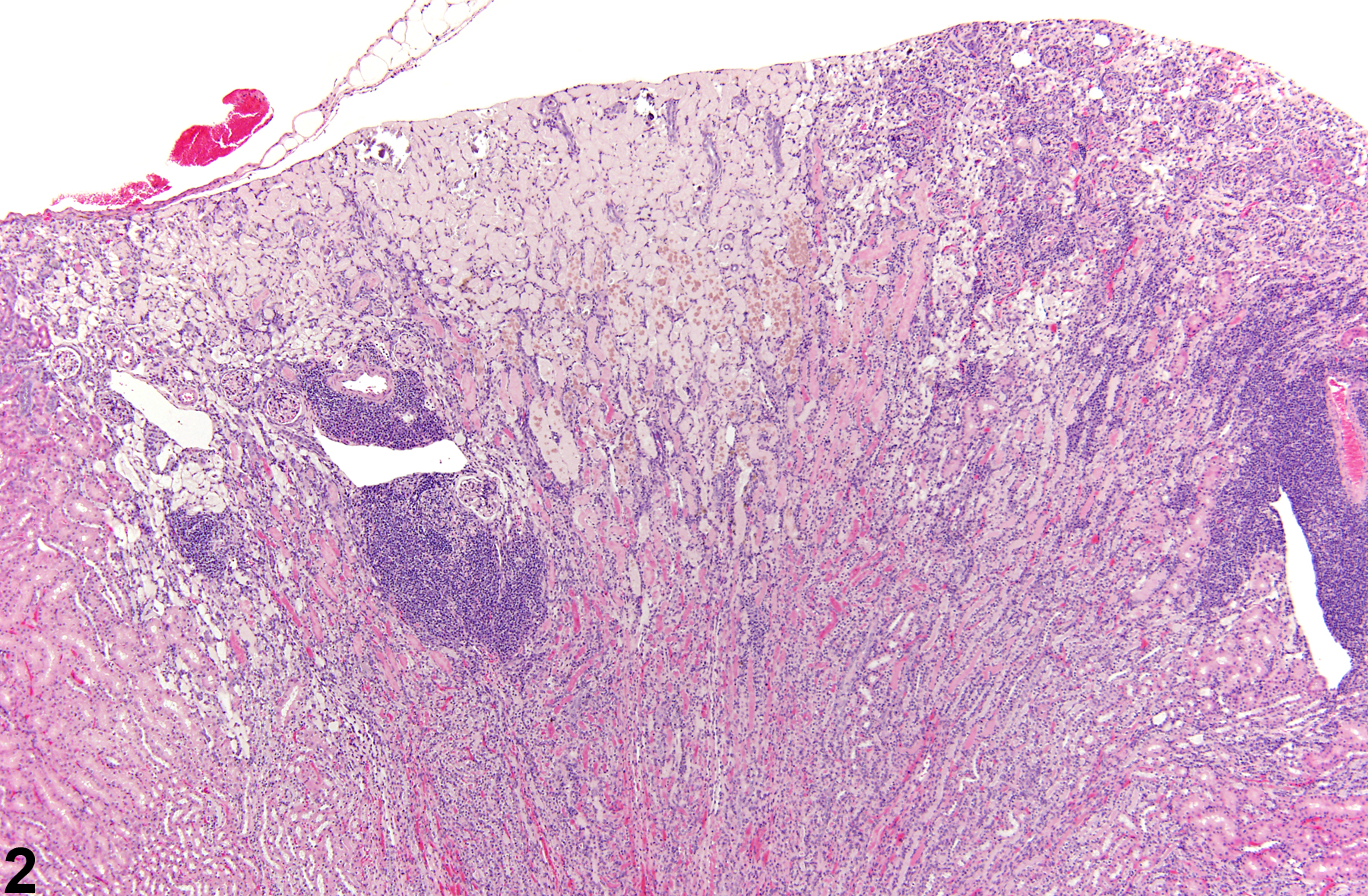
Kidney - Infarct in a female F344/N rat from a chronic study. A wedged-shaped cortical area of acute coagulative necrosis is present.
All Images

Kidney - Infarct in a female F344/N rat from a chronic study. A wedged-shaped cortical area of acute coagulative necrosis is present.

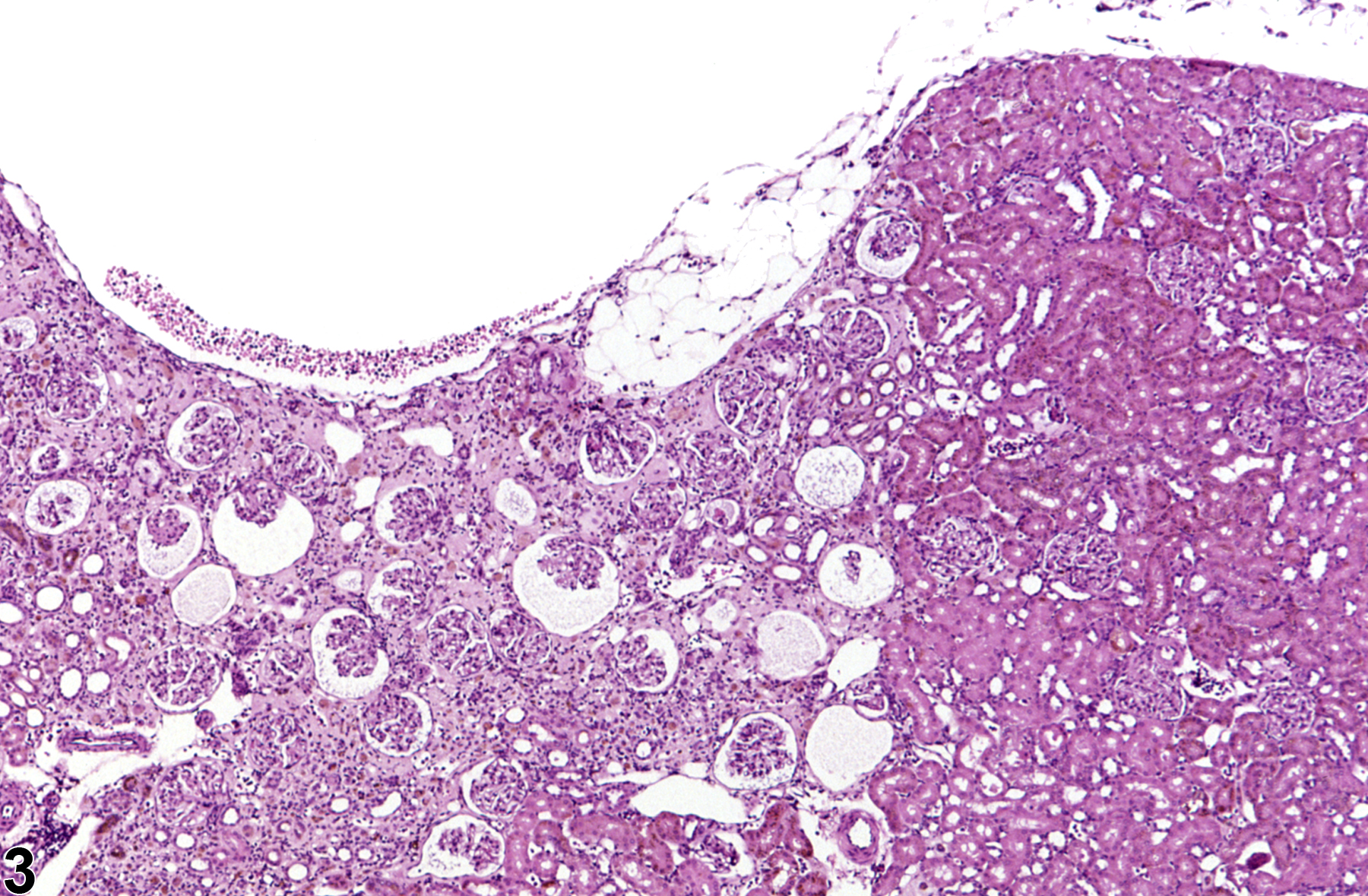
Kidney - Infarct in a female B6C3F1 mouse from a chronic study. This infarct has a prominent area of basophilic inflammatory cellularity associated with an infarcted area.

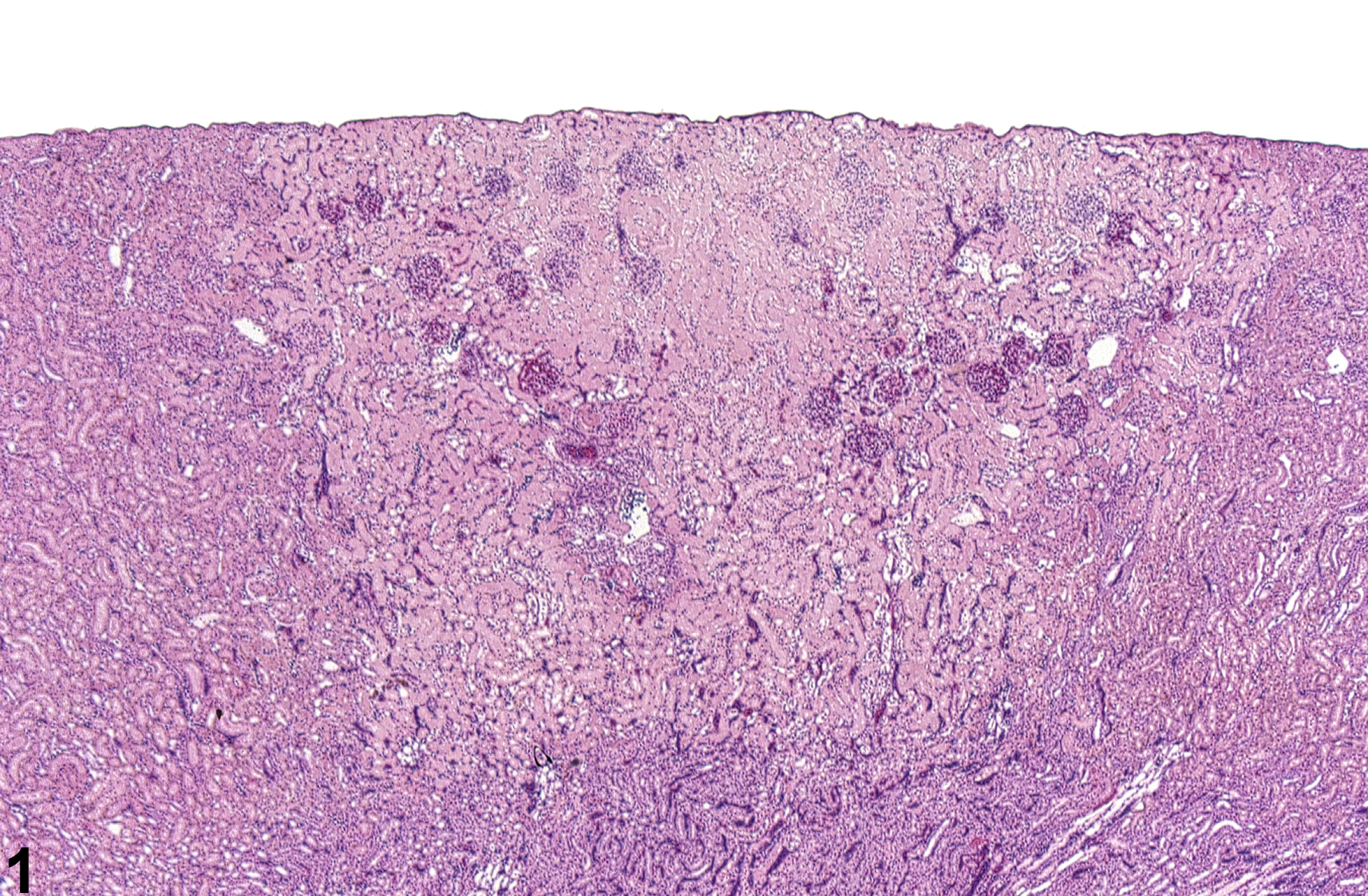
Kidney - Infarct in a female B6C3F1 mouse from a chronic study. This chronic or healed infarct is characterized by cortical depression and interstitial fibrosis.