

Respiratory System
Lung, Epithelium - Necrosis
Narrative
{kind=link}
{kind=link}
{kind=link}
The anatomic location of necrotic lesions may vary due to the physicochemical properties of the test agent or the susceptibility of a particular cell type to the test agent. The epithelium of the terminal bronchioles and alveolar ducts (i.e., the centriacinar region) and alveoli are particularly susceptible to injury due to the large surface area and fragility of the alveolar type I cells, the metabolic activity of P450 enzymes in Clara cells, and the generally thinner mucous layer.
Boorman GA, Eustis SL. 1990. Lung. In: Pathology of the Fischer Rat: Reference and Atlas (Boorman GA, Eustis SL, Elwell MR, Montgomery CA, MacKenzie WF, eds). Academic Press, San Diego, CA, 339-367.
Haschek-Hock WM, Witschi HP. 1990. Respiratory system. In: Handbook of Toxicologic Pathology (Haschek-Hock WM, CG Rousseaux, eds). Academic Press, San Diego, CA, 761-827.
Kumar V, Abbas AK, Fausto N. 2005. Cellular adaptations, cell injury, and cell death. In: Robbins and Cotran Pathologic Basis of Disease, 7th ed. Elsevier Saunders, Philadelphia, 3-48.
Lopez A. 2007. Respiratory system. In: Pathologic Basis of Veterinary Disease, 4th ed (McGavin MD, Zachary JF, eds). Mosby, St Louis, 463-558.
Plopper CG, Dungworth DL. 197. Structure, function, cell injury and cell renewal of bronchiolar and alveolar epithelium. In: Lung Carcinomas (McDowell EM, ed). Churchill Livingstone, Edinburgh, 94-128.
Renne, R, Brix A, Harkema J, Herbert R, Kittle B, Lewis D, March T, Nagano K, Pino M, Rittinghausen S, Rosenbruch M, Tellier P, Wohrmann T. 2009. Proliferative and nonproliferative lesions of the rat and mouse respiratory tract. Toxicol Pathol 37(suppl):5S-73S.
Abstract: https://www.ncbi.nlm.nih.gov/pubmed/20032296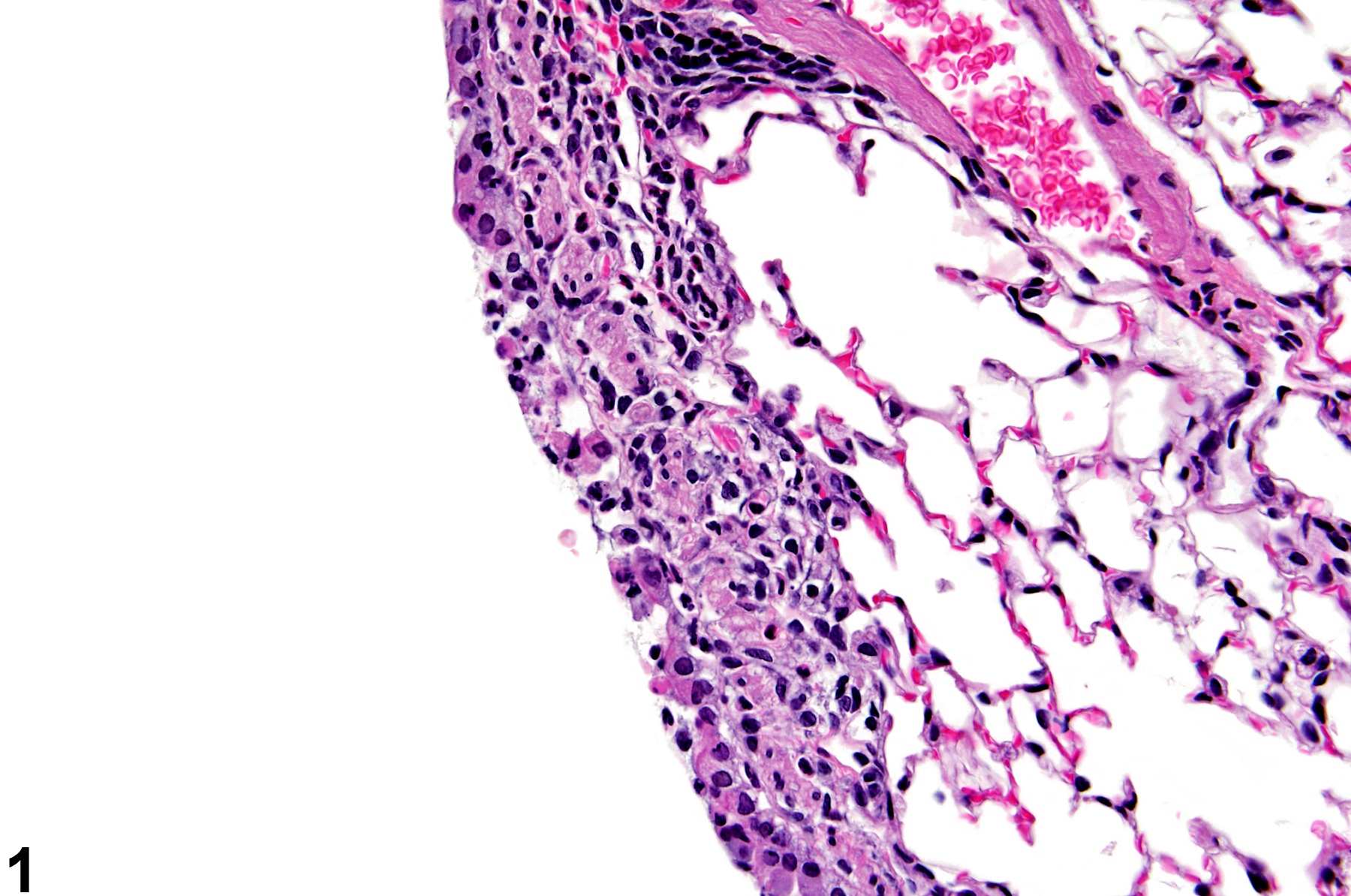
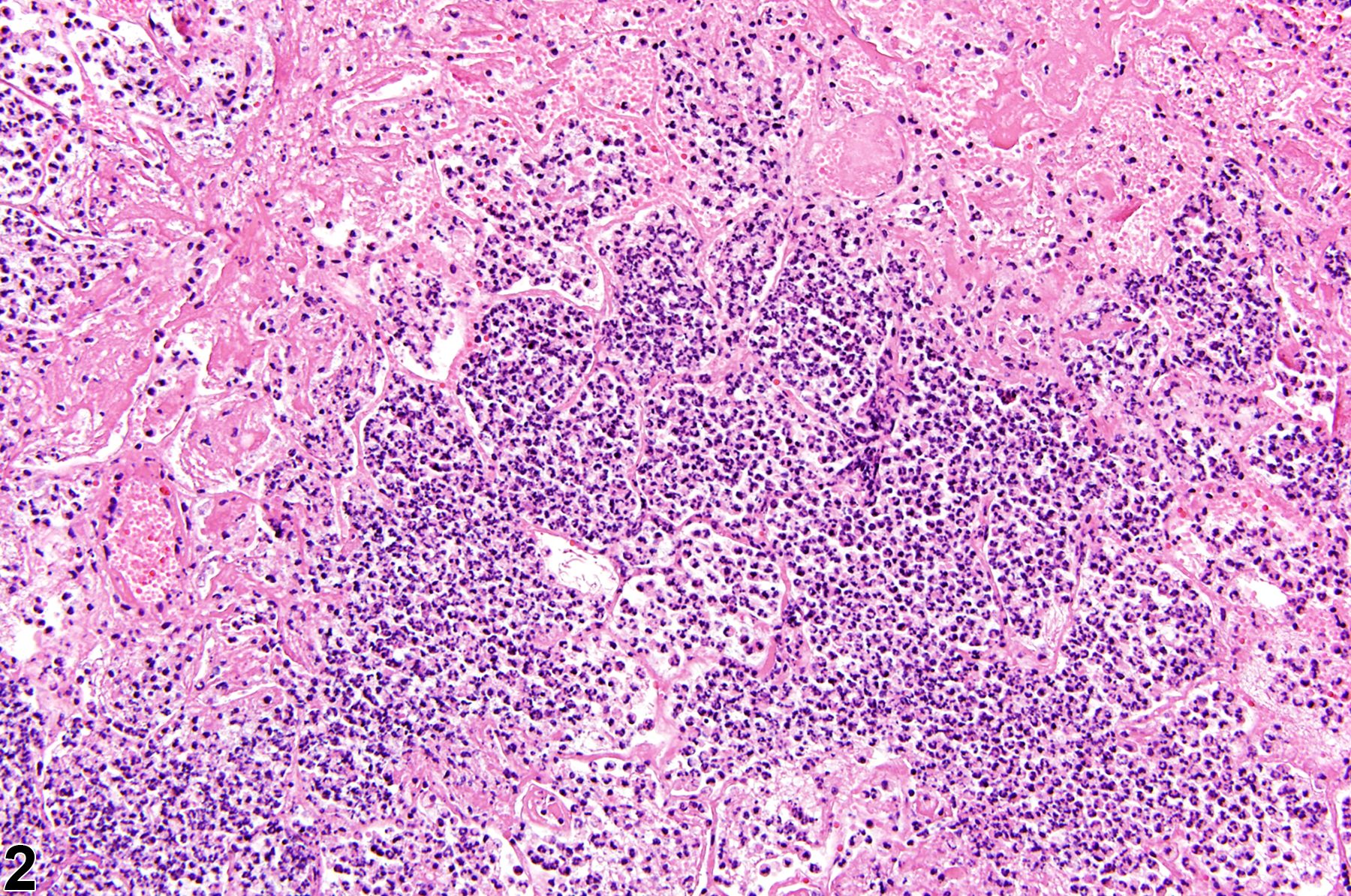
Lung, Bronchiole, Epithelium, Bronchiole - Necrosis in a female B6C3F1/N mouse from a subchronic study. The epithelial cells are fragmented, with pyknotic and karyorrhectic nuclei.
All Images

Lung, Bronchiole, Epithelium, Bronchiole - Necrosis in a female B6C3F1/N mouse from a subchronic study. The epithelial cells are fragmented, with pyknotic and karyorrhectic nuclei.

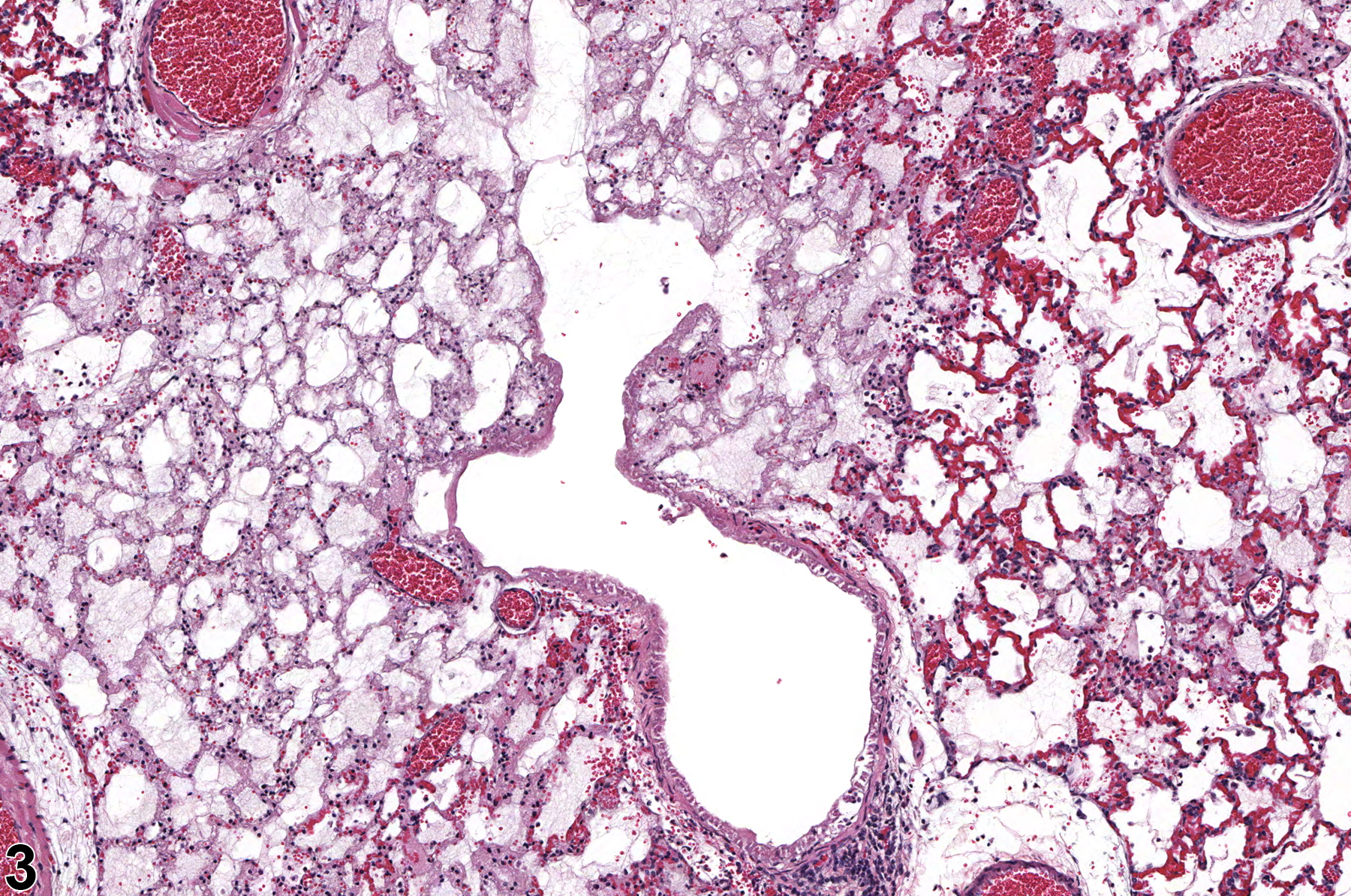
Lung, Epithelium - Necrosis in a male Wistar Han rat from a chronic study. There is a large area of coagulative necrosis surrounded by suppurative inflammation.

Lung, Epithelium, Alveolus - Necrosis in a female F344/N rat from a subchronic study. There is loss of epithelial cells, and many of the interstitial cells have pyknotic nuclei.

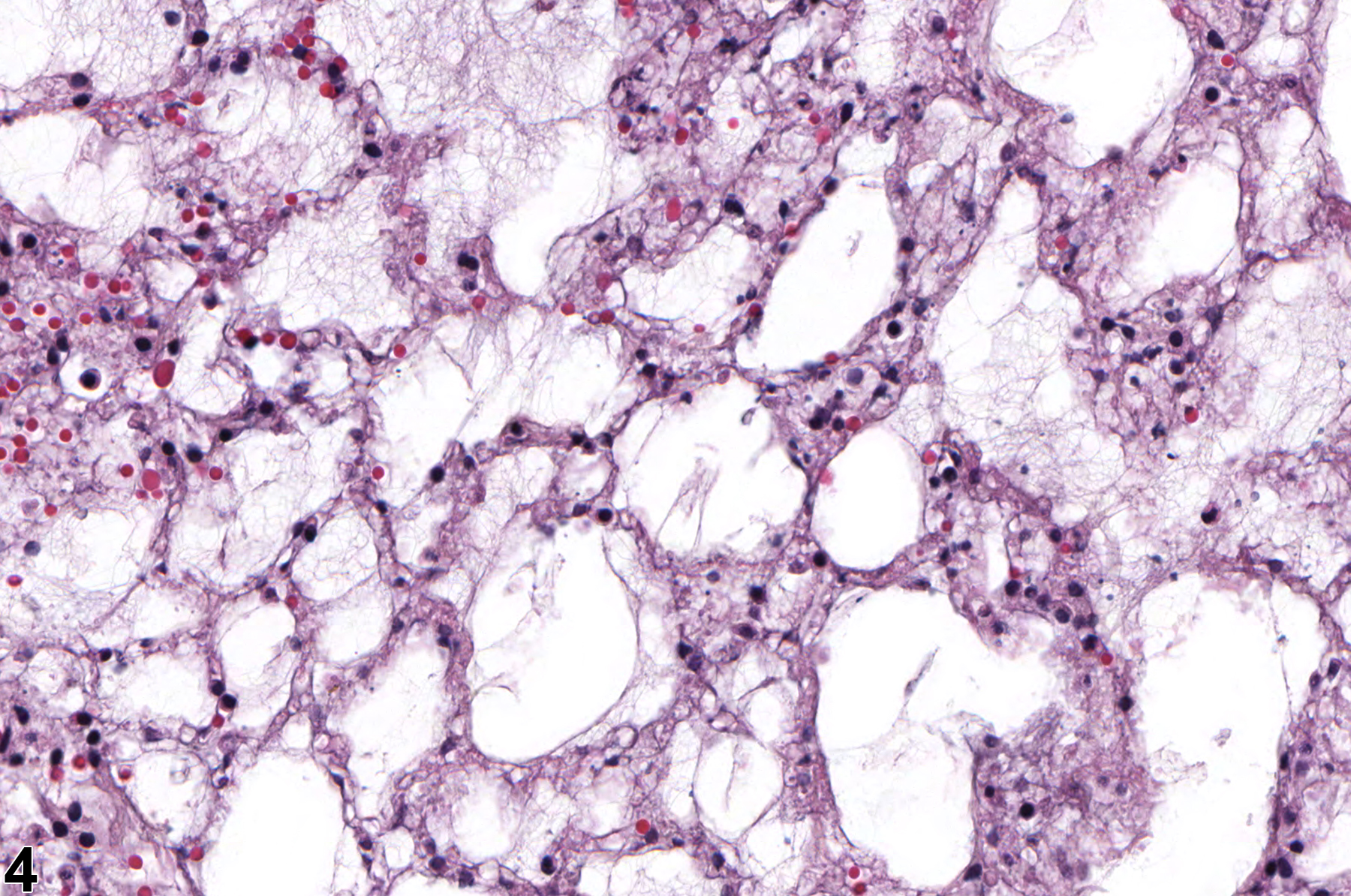
Lung, Epithelium, Alveolus - Necrosis in a female F344/N rat from a subchronic study. In this focal lesion, there is loss of epithelial and interstitial cells.